
How EMDR Uses Working Memory: The Mechanism Behind Bilateral Stimulation
- Kiesa Kelly

- May 9
- 12 min read
Last reviewed: 05/09/2026
Reviewed by: Dr. Kiesa Kelly

You have heard EMDR is "moving your eyes back and forth while you think about something hard," and you want to know whether that is actually doing anything. Maybe a clinician suggested it after a PCL-5 screening came back high. Maybe you have done years of talk therapy and the memory you keep circling still has the same charge it always had. Either way, the mechanism question matters — knowing why bilateral stimulation works (or is hypothesized to work) shapes what to expect in session and helps you recognize when reprocessing is going right.
This article walks through the leading mechanistic theory for how EMDR's bilateral stimulation reduces the vividness and emotional charge of trauma memories: the working memory taxation hypothesis. It is not the only theory, and the field treats the mechanism as multi-pathway rather than settled. But the working memory account is the most empirically supported, and it explains some clinically useful patterns that any other story would need to explain too.
In this article, you'll learn:
Why the mechanism question is real, not a stalling tactic
What working memory is and why it has a fixed capacity ceiling
How the working memory taxation hypothesis explains EMDR's effect
What the research base actually shows — and where it is still being refined
What this means for what you should expect in your sessions
Why "how does EMDR work" is a real question
People who ask how EMDR works are sometimes assumed to be stalling — wanting one more reason not to start. In our practice, the opposite is more often true. Adults who ask this question want to feel the work makes sense before they sit through hours of revisiting hard material. Understanding the mechanism is part of how some people give consent to a therapy that, on the outside, looks weird.
The mechanism question also matters clinically. Knowing why bilateral stimulation works helps you spot when a session is on track (decreasing distress and vividness) versus when something else is going on (rising distress, dissociation, or shutdown — which signals a need to slow down or stabilize first). Mechanism understanding is not just intellectual cover; it's part of how the work gets paced safely.
What working memory is
Working memory is the mental scratchpad — the small holding space your brain uses to keep information active while you do something with it [1]. It is what lets you remember a phone number long enough to dial it, hold the start of a sentence in mind while you finish reading the rest, or keep the goal of a task active while you work through the steps.
Three things matter about working memory for the EMDR story:
It has a limited capacity. Most adults can hold only a handful of items at once before something gets dropped [1]. The capacity is not adjustable through effort.
It is shared. Visualizing an image and tracking a moving target both draw on the same general-purpose working memory resources, especially the visuospatial subsystem [1,2]. Doing both at once means each is competing for the same limited slot.
It is the place where vivid recall lives. When you remember a hard event, the sensory and emotional details are reconstructed in working memory — they don't simply replay from a file. That reconstruction is what makes a memory feel vivid and present, and it is what taxes the system the same way any other cognitively demanding task does [2].
This combination — limited capacity, shared resources, the home of vivid recall — is what the working memory taxation hypothesis builds on.
Three things people often get wrong about EMDR's mechanism
Before reading further, it helps to clear three misconceptions that keep readers stuck.
EMDR works by erasing the memory. In reality, EMDR does not delete or overwrite the memory. The event still happened, and you still remember it. What changes is the vividness and emotional intensity of the recall. Studies consistently show reductions in self-reported memory vividness and distress after reprocessing, not changes to the factual recall itself [2,3]. Reprocessing makes the memory feel like a memory rather than a present-tense event.
The eye movements are doing something special and unique. In reality, lab and clinical research find that the modality of bilateral stimulation matters less than the dual-attention task itself [2]. Eye movements, alternating taps, and alternating tones all show similar effects on memory vividness when they tax working memory. What is doing the work is the simultaneous load on working memory, not the eyes specifically. This is why telehealth EMDR with self-tapping or audio tones can work clinically — the load is what matters.
EMDR is just exposure with extra steps. In reality, EMDR and prolonged exposure (PE) have meaningfully different procedural elements. PE asks you to stay with the trauma memory for extended periods at high distress to allow extinction learning [4]. EMDR holds the image in mind only briefly while taxing working memory, which appears to reduce vividness through a different mechanism than habituation. Both are first-line, evidence-based treatments for PTSD per current guidelines [4,5], but they are not interchangeable techniques.
The working memory taxation hypothesis
The working memory taxation hypothesis says, roughly, this: when you recall a hard memory in vivid detail, that recall consumes working memory capacity. When you simultaneously do a task that also consumes working memory (tracking eye movements, following bilateral taps, attending to alternating tones), there is less capacity available for the vivid recall. The memory's vividness drops because the resource it needed to be vivid is being used elsewhere [2,6].
What changes with repeated dual-attention exposure is durable rather than just momentary. After the dual-task exposure, recalling the memory under ordinary conditions consistently produces less vivid imagery and lower distress than before — a learning effect that persists between sessions and across time [2,6]. The mechanism is hypothesized to involve memory reconsolidation: the memory, having been retrieved in a state of reduced vividness, is re-stored with less of its prior emotional charge [3].
A worked example helps. You are asked to bring up a specific traumatic memory and rate its vividness from 0 to 10 — let's say you rate it 8. You then begin tracking bilateral stimulation while holding the image in mind. The dual task uses working memory resources, leaving less capacity for the vivid reconstruction. After 30–60 seconds, the clinician pauses and asks you to rate vividness again — it has dropped to 5. Repeated cycles further reduce the vividness, and what is re-stored is the lower-vividness version of the memory.
This is what a clinician means when they say EMDR "reprocesses" a memory: not editing the content, but reducing the emotional charge attached to retrieval — through a working-memory-mediated reconsolidation pathway [3].
Key takeaway: 🧠 The mechanism is not magic and is not the eyes. It is dual-task load on working memory, plus repeated retrieval at reduced vividness, plus reconsolidation. Eye movements happen to be one effective form of the load; tapping and tones can do the same job.
What the research actually shows
The working memory account is empirically well supported but not the whole story. A few things the literature consistently demonstrates:
Across modalities. Eye movements, alternating taps, and audio tones all reduce memory vividness when they tax working memory simultaneously [2]. Studies that vary the modality but hold the dual-task structure constant find similar effects.
Capacity-load matters. Tasks that load working memory more heavily produce larger vividness reductions, up to a ceiling — beyond a certain load, recall starts to fail entirely (you can't keep the image in mind), which is why clinicians titrate the speed and complexity of bilateral stimulation rather than maxing it [2].
Effects persist. Vividness reductions outlast the dual-task period; follow-up sessions show maintained reductions, consistent with a reconsolidation-style mechanism rather than a momentary distraction effect [3].
Clinical efficacy is established. Multiple meta-analyses and clinical practice guidelines list EMDR as a first-line, evidence-based treatment for PTSD across populations [4,5]. The mechanism question is a separate research question from the efficacy question — efficacy is settled even where mechanism is still being refined.
What is contested or not yet settled:
Whether the working memory model is the only mechanism. REM-like neural processes, adaptive information processing (AIP) models, and changes in attention and memory networks have all been proposed as additional or alternative mechanisms [6]. Most researchers now treat the mechanism as multi-pathway — the working memory account is the best supported, but it likely is not the entire picture.
Why some adults respond more strongly than others. Predictors of strong EMDR response are not fully mapped; clinical factors (preparation, stability, complex trauma history) interact with the dual-task mechanism in ways the working memory account alone does not predict.
We treat the working memory taxation hypothesis as the leading mechanistic story, while acknowledging the field is still building consensus on the broader question.
What this means for your sessions
Three things follow from the mechanism that show up in how EMDR is paced.
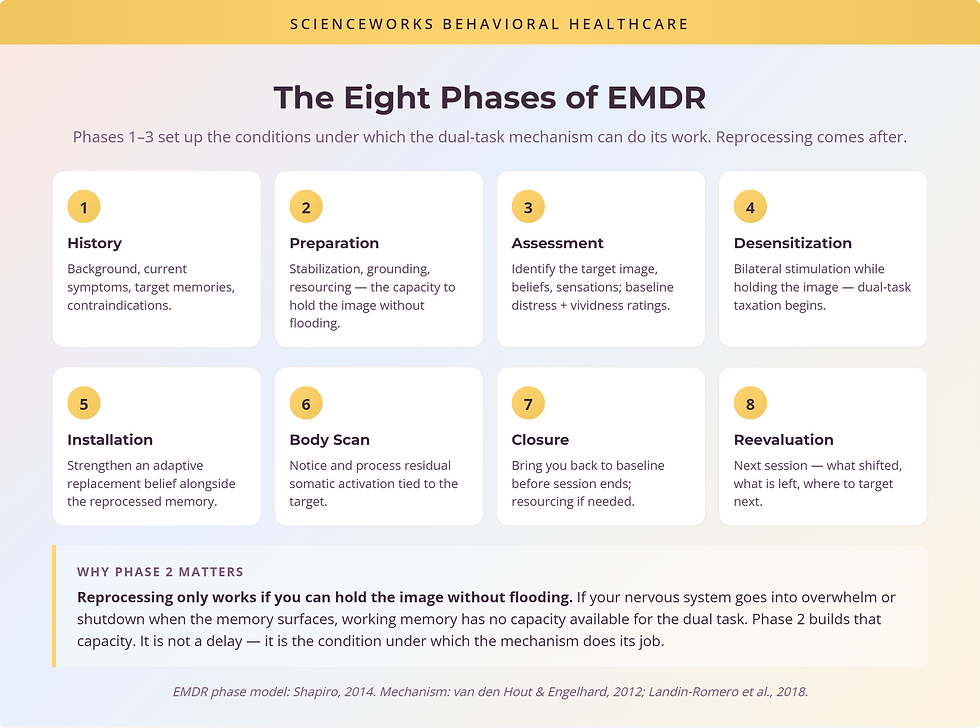
Why phases 1–3 come before any reprocessing. Before bilateral stimulation begins, an EMDR clinician spends time on history, preparation, resourcing, and target selection — often several sessions, sometimes more for complex-trauma cases. From a working memory perspective, this matters because the dual-task mechanism only works when you can hold the image in mind without flooding. If your nervous system goes into overwhelm or shutdown the moment the memory surfaces, you have no working memory available for the dual task — and reprocessing becomes destabilizing rather than therapeutic. The preparation phase builds the capacity to do the dual task safely.
Why bilateral stimulation should not feel relaxing. Bilateral stimulation is supposed to tax your working memory. If the speed, modality, or complexity of stimulation is too low, no taxation happens — and no vividness reduction follows. A skilled clinician titrates the bilateral stimulation to your capacity: enough load to do the work, not so much that you lose the image. If a session feels uniformly easy, the dual task is probably under-loading. If it feels overwhelming, it is over-loading. The working zone is structured effort, not relaxation.
Why memory vividness drops before distress does. In session, vividness usually drops first — the memory loses its present-tense, surround-sound quality — and the emotional charge attached to recall follows. Adults sometimes notice this as "I can still describe what happened, but it does not grab me anymore." That sequence is consistent with the working-memory-then-reconsolidation pathway: the resource competition reduces vividness in the moment, repeated cycles reinforce the lower-vividness version, and the emotional charge attached to the lower-vividness memory is correspondingly reduced.
Key takeaway: 🌊 Pacing is the work. Slow phases 1–3, titrated bilateral stimulation, and patient cycles are not delays — they are the conditions under which the dual-task mechanism actually does what it does.

Where the working memory model isn't the whole story
A few honest limits of the dominant theory:
REM-like and consolidation models. Some researchers propose that bilateral stimulation produces neural states resembling REM sleep, where memory consolidation processes naturally re-encode emotional memories [6]. The working memory account does not fully explain the across-session durability of EMDR effects on its own; consolidation models add explanatory weight there.
Adaptive Information Processing (AIP). EMDR's foundational clinical model — Shapiro's AIP framework — describes how adaptively-processed memories integrate with existing networks [3]. AIP is a clinical model, not a competing mechanistic theory in the lab-research sense, but it shapes how clinicians think about case formulation and target sequencing in ways the working memory account does not.
Attentional and emotional regulation pathways. Some lines of research focus on how bilateral stimulation engages attention and emotion regulation networks specifically — a related but distinct mechanism from generic working memory load [6].
The field's current posture: the working memory account is the most empirically supported single mechanism, but treating EMDR's effects as multi-pathway is more accurate than treating any single theory as complete. None of this changes the clinical efficacy, which is independently established across multiple meta-analyses [4,5].
When EMDR is and isn't the right starting point
A short decision frame, framed by the mechanism story:
If your trauma is one or a few discrete events and you are stable enough to hold the memory without flooding, EMDR is often a strong starting point. The dual-task mechanism is well-suited to discrete-event reprocessing.
If your history is long, layered, or includes dissociation, an extended Phase 2 (preparation, stabilization, resourcing) before any reprocessing matters — sometimes weeks to months. EMDR with a clinician trained in complex-trauma work can still be useful; the pacing differs.
If you are currently in crisis, actively unsafe, or unable to maintain dual attention without flooding, the working memory mechanism cannot do its job in that state. Stabilization-focused work usually comes first.
If your first-line trauma question is settled and you are looking for a clinician fit, trauma services and specialized therapy are the entry points — both routes lead to clinicians trained to evaluate whether EMDR is the right opening modality for your specific picture.
Questions worth asking before booking
If the mechanism makes sense to you and you are considering EMDR, these questions help you sort fit before you commit:
Training and approach. "What is your specific EMDR training and certification, and how do you think about phase 2 preparation for adults with longer histories or dissociation?"
Telehealth fit. "Do you offer EMDR over telehealth? What bilateral stimulation modality do you use remotely, and how do you decide whether telehealth is appropriate for a given client?"
Pacing and stability. "How do you decide when a client is ready to begin reprocessing? What signs tell you we should slow down or stay in stabilization longer?"
Integration with other modalities. "If EMDR isn't the right starting point or stalls for me, what other modalities do you use, and how do you sequence them?"
These questions matter because EMDR fit depends as much on clinician training and case formulation as on diagnosis. A clinician who answers them comfortably is doing the kind of pacing the mechanism actually requires.
Schedule a consult
If you are weighing EMDR for trauma or PTSD, a consult is the cleanest first step. We can talk through your history, the current symptom picture, and whether EMDR is the right opening move — or whether stabilization, a different modality, or a sequence of approaches makes more sense for your specific situation.
Frequently Asked Questions
Does EMDR have to use eye movements?
No. The bilateral stimulation can be eye movements, alternating taps on the knees or shoulders, or alternating audio tones through headphones. Lab and clinical research consistently finds that the modality of stimulation matters less than the dual-attention task itself — what reduces the vividness of a recalled memory is taxing working memory while holding the image in mind. Many adults find tapping or tones easier than tracking eye movements, especially for telehealth sessions.
Can EMDR be done over telehealth?
Yes. Telehealth EMDR uses on-screen visual targets, alternating tones, or self-administered tapping (the 'butterfly hug') as the bilateral stimulation. Outcomes in clinical settings have generally been comparable to in-person EMDR for many adults, though clinicians screen carefully for stability and dissociation risk before recommending remote work for a given case. The clinician's training matters more than the medium.
Does EMDR erase the traumatic memory?
No. EMDR does not delete or rewrite the memory itself. What changes during reprocessing is the vividness, distress, and emotional charge attached to the memory — the event still happened, and you still remember it, but recalling it no longer hits with the same force. Many adults describe the memory as 'distant' or 'in the past where it belongs' after reprocessing, while still able to talk about it accurately.
How long does it take to feel a difference?
It varies. Some adults notice a shift in distress within one or two reprocessing sessions on a single discrete event; complex or layered trauma usually takes longer — months of work across multiple targets is more typical. Phases 1–3 (history, preparation, target selection) often take several sessions before any reprocessing begins, which is part of why EMDR is paced rather than rushed. Pacing is protective, not a delay.
Is EMDR appropriate for complex trauma or dissociation?
Sometimes, with caveats. Complex trauma and dissociative presentations need extended preparation in Phase 2 — building stabilization, grounding, and resourcing skills before any reprocessing begins. Some people benefit greatly from EMDR with a clinician trained in complex-trauma work; others do better with a different first-line trauma modality. The right fit depends on history, current stability, and clinician training, not on the diagnosis label alone.
About the Author
Dr. Kiesa Kelly is a licensed clinical psychologist with more than 20 years of experience in psychological assessment and evidence-based treatment. Her clinical training and research foundations include trauma-focused care, neurodevelopmental assessment, and evidence-based treatment for adults across the lifespan, with formal advanced training at the University of Chicago, Vanderbilt University, and the University of Wisconsin.
Dr. Kelly leads psychological assessment and clinical oversight at ScienceWorks Behavioral Healthcare, where the practice's trauma services include EMDR alongside other evidence-based modalities for adults with single-event and complex trauma histories. Her work emphasizes paced, mechanism-aware care that respects the reader's capacity rather than rushing reprocessing.
References
1. Baddeley A. Working memory: theories, models, and controversies. Annu Rev Psychol. 2012;63:1-29. https://doi.org/10.1146/annurev-psych-120710-100422
2. van den Hout MA, Engelhard IM. How does EMDR work? J Exp Psychopathol. 2012;3(5):724-738. https://doi.org/10.5127/jep.028212
3. Shapiro F. The role of eye movement desensitization and reprocessing (EMDR) therapy in medicine: addressing the psychological and physical symptoms stemming from adverse life experiences. Perm J. 2014;18(1):71-77. https://doi.org/10.7812/TPP/13-098
4. American Psychological Association. Clinical practice guideline for the treatment of posttraumatic stress disorder (PTSD) in adults. 2017. https://www.apa.org/ptsd-guideline
5. World Health Organization. Guidelines for the management of conditions specifically related to stress. 2013. https://www.who.int/publications/i/item/9789241505406
6. Landin-Romero R, Moreno-Alcazar A, Pagani M, Amann BL. How does eye movement desensitization and reprocessing therapy work? A systematic review on suggested mechanisms of action. Front Psychol. 2018;9:1395. https://doi.org/10.3389/fpsyg.2018.01395
7. Cuijpers P, Veen SCV, Sijbrandij M, Yoder W, Cristea IA. Eye movement desensitization and reprocessing for mental health problems: a systematic review and meta-analysis. Cogn Behav Ther. 2020;49(3):165-180. https://doi.org/10.1080/16506073.2019.1703801
8. Bisson JI, Roberts NP, Andrew M, Cooper R, Lewis C. Psychological therapies for chronic post-traumatic stress disorder (PTSD) in adults. Cochrane Database Syst Rev. 2013;(12):CD003388. https://doi.org/10.1002/14651858.CD003388.pub4
9. Maxfield L, Melnyk WT, Hayman GCA. A working memory explanation for the effects of eye movements in EMDR. J EMDR Pract Res. 2008;2(4):247-261. https://doi.org/10.1891/1933-3196.2.4.247
10. National Institute for Health and Care Excellence. Post-traumatic stress disorder (NG116). 2018. https://www.nice.org.uk/guidance/ng116
Disclaimer
This article is for informational and educational purposes only. It is not medical advice and is not a substitute for an evaluation by a licensed clinician. Reading this article does not establish a clinician-patient relationship with Dr. Kelly or with ScienceWorks Behavioral Healthcare. If you are experiencing distress that disrupts your day-to-day life or have a recent traumatic event, talk with a qualified clinician about the right next step for your situation.