
Misophonia in Autistic Adults: The Sensory Overlap Clinicians Watch For
- Kiesa Kelly

- 2 days ago
- 12 min read
Last reviewed: 06/26/2026
Reviewed by: Dr. Kiesa Kelly

If a family member's chewing makes your whole body tense, or a coworker's pen-clicking pulls your attention into a spiral of anger you cannot talk yourself out of, you are not being dramatic and you are not "too sensitive." You may be describing misophonia — a real, well-documented condition in which specific everyday sounds set off an immediate, intense emotional and physical reaction. For autistic adults, this is especially common, and it often gets folded into the broader story of "sensory issues" without anyone naming what is actually happening.
Misophonia in autistic adults sits at the overlap of two things that are easy to confuse: a sound-specific reaction and a general sensory load. Telling them apart matters, because it changes what helps.
In this article, you'll learn:
What misophonia is, and how it differs from autistic sensory overload and hyperacusis
How common misophonia is among autistic adults, and why the two overlap
What an evaluation looks at — and what it rules in or out
What the brain is actually doing during a trigger reaction
Which approaches have evidence behind them, and which to be cautious of
When it is worth seeking a formal assessment
What misophonia is — the short answer
Misophonia is a strong, involuntary aversion to particular sounds — most often human-generated ones like chewing, slurping, swallowing, breathing, sniffing, tapping, or pen-clicking [1]. The reaction is fast and disproportionate to the volume: a quiet sound can produce a flood of anger, disgust, panic, or the urge to flee or lash out. People describe it as a hijacking — the feeling arrives before any thought does.
This is different from simply disliking a sound. With misophonia, the trigger reliably produces a specific emotional and bodily response that interferes with daily life — meals with family, open-plan offices, relationships. A 2022 international expert panel formally defined it as a disorder of decreased tolerance to specific sounds, distinct from ordinary noise annoyance and from hearing disorders [2]. Naming it is recent; the experience is not.
For autistic adults, misophonia frequently rides alongside the broader pattern of sensory overload and overstimulation, but it is not the same mechanism — and that distinction is the first thing worth getting straight.
Three misconceptions worth clearing up first
Because misophonia is newly defined and often misread, a few wrong ideas tend to keep people stuck. It helps to name them directly.
"It's just being oversensitive — you need to toughen up." In reality, misophonia is not a willpower problem or a matter of attitude. Brain-imaging research shows trigger sounds produce abnormal activity in the anterior insula and exaggerated links to threat-processing regions, with measurable spikes in heart rate and skin conductance [3]. The reaction is physiological — telling someone to ignore it is like telling them to ignore a sudden burn.
"If you can wear headphones at a concert, it can't be a real sound problem." Misophonia is not about loudness. A barely audible chewing sound across a room can trigger a severe reaction while a loud concert feels fine. The brain is responding to the meaning and pattern of specific sounds, not their decibel level — which is exactly why it confuses people who assume all sound sensitivity is about volume.
"It's the same as autistic sensory overload, so there's nothing separate to treat." These overlap but differ in mechanism, and treating them as identical leaves real options on the table. Sensory overload is the cumulative result of too much input at once; misophonia is a targeted reaction to particular sounds. A reader can be flooded by a busy grocery store (overload) and also unravel at a single repetitive tapping sound in a silent room (misophonia). Recognizing both means you can address each on its own terms.
🧩 Key takeaway: Misophonia is a sound-specific, physiologically real reaction — not a volume problem, a character flaw, or simply a synonym for sensory overload.
How misophonia shows up in autistic adults
Core features
The hallmark is a consistent set of trigger sounds that reliably produce an outsized reaction. In autistic adults, the trigger list is often longer and the threshold lower, because the nervous system is already managing a heavier baseline sensory load. The most commonly reported triggers are oral sounds — chewing, slurping, and swallowing — followed by breathing, throat-clearing, tapping, and repetitive clicking [1]. Visual versions exist too: some people react to the sight of a repetitive movement, like a jiggling leg.
The reaction usually moves through stages: an instant spike of irritation or disgust, a surge of anxiety or anger, a strong urge to escape or make the sound stop, and then often guilt — especially when the trigger is a person you love. For autistic adults already working hard to regulate in a world built for a different nervous system, this adds another layer of effort and shame that rarely gets spoken aloud.
How it shows up day to day
Consider a recognizable week. You can manage a loud, chaotic morning commute because the noise is broad and impersonal, but the moment a colleague starts eating crackers at the next desk, your attention locks onto the sound and will not let go. You cannot follow the meeting. You feel your jaw clench and your heart speed up. You spend forty minutes rehearsing how to ask them to stop without seeming hostile, and by lunch you are exhausted in a way that has nothing to do with the work itself.
Or: family dinner is the hardest hour of your day. You love these people, and yet the sound of chewing makes your skin crawl and your temper rise. You have started eating earlier, alone, or with your own headphones in, and you carry quiet guilt about the distance it creates. You have wondered whether something is wrong with you for reacting this strongly to the people you most want to be close to.
These are recognizable misophonia patterns, not overreactions, and they often coexist with the attention and regulation differences seen in ADHD — which is why the overlap with misophonia and ADHD is worth understanding if both feel familiar. If you have never had your neurodevelopmental profile assessed, a screener like the AQ-10 is a low-stakes place to start.
🔊 Key takeaway: In autistic adults, misophonia triggers tend to be more numerous and the threshold lower, because the sound reaction lands on top of an already-taxed sensory system.
Why misophonia and autism overlap
This is not just clinical impression. A 2025 systematic review pooling fourteen studies and nearly 90,000 participants estimated that misophonia occurs in roughly 12.8% to 35.5% of autistic people, well above general-population estimates [1]. From the other direction, studies of people with misophonia find elevated autistic traits and broad sensory hypersensitivity compared with controls — visible across attention, communication, social, and sensory domains, and present even in children aged 10 to 14 [4].
A likely reason is shared wiring. Autism involves differences in how the brain filters and integrates sensory information, and misophonia appears to involve heightened threat-tagging of specific sounds in the same insula-centered circuitry [3]. When a system is already primed to register sensory detail intensely, a sound-specific reaction has fertile ground to take hold. That shared substrate is also why misophonia rarely travels alone: the same review found about 79% of autistic individuals with misophonia also met criteria for another psychiatric condition, most often anxiety, OCD, or depression [1].
That comorbidity matters for care, because untreated anxiety or OCD lowers your tolerance for triggers. If checking, intrusive thoughts, or compulsions are part of your picture, a Y-BOCS screen can clarify whether OCD is in the mix, and the energy cost of constant sensory management is closely related to autistic burnout. Mapping what else is going on is how you find the pieces that are actually treatable.
🧠 Key takeaway: Misophonia is meaningfully more common in autistic adults, likely because both involve heightened sensory salience — and it usually co-occurs with anxiety, OCD, or depression.
How misophonia is assessed
What an evaluation looks at
There is no single blood test or brain scan that diagnoses misophonia. A careful clinical assessment instead builds a detailed picture: which sounds trigger you, how intense and consistent the reactions are, how much they interfere with work, relationships, and daily life, and how long the pattern has been present.
For autistic adults specifically, the assessment should account for masking and lifelong compensation. Many adults have spent years quietly rearranging their lives around triggers — eating alone, avoiding certain rooms, scripting requests — so the surface picture can look "managed" even when the internal cost is high. A clinician who understands this will ask about the workarounds, not just the meltdowns. Our psychological assessments take that fuller history rather than treating sound reactions in isolation.
What rules it in or out
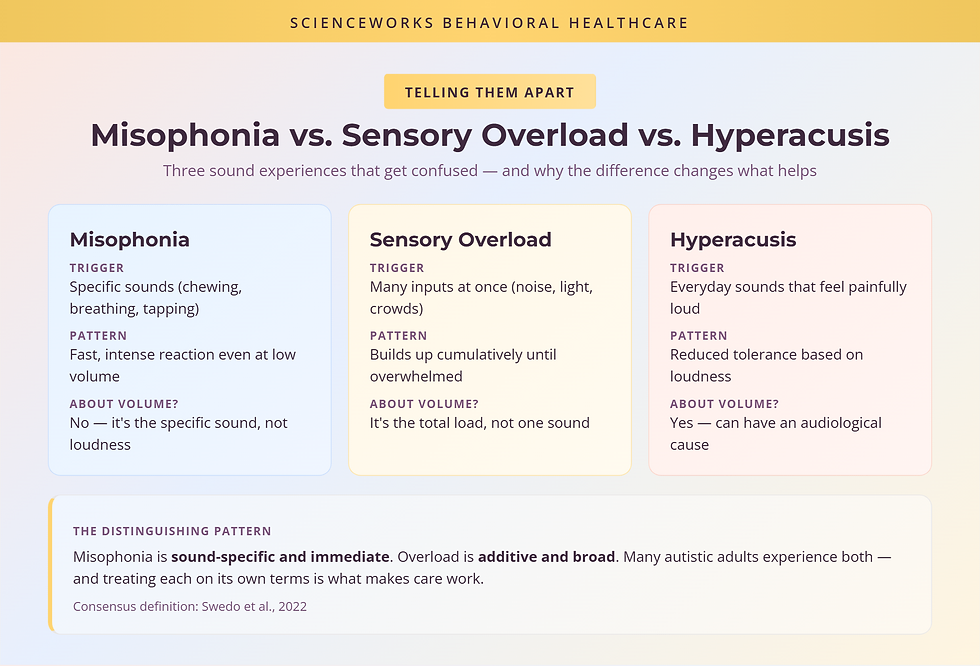
Part of a good assessment is distinguishing misophonia from conditions it resembles. Hyperacusis is a reduced tolerance to sound based on volume — ordinary sounds feel painfully loud — and it can have an audiological cause; misophonia, by contrast, is about specific sound patterns regardless of loudness [2]. Sensory overload is the broad, additive flooding many autistic adults know well, where the issue is the total volume of input rather than one repeated trigger. And ordinary irritation at an annoying noise is transient and does not reliably produce the same intense, patterned response.
A thorough evaluation also screens for co-occurring anxiety, OCD, and depression, since these shape both the experience and the treatment plan. If you are not sure where your reactions fit, our mental health screening overview can help you sort the threads before a full appointment.
📋 Key takeaway: Assessment is clinical and history-based — it separates misophonia from hyperacusis and general overload, and it screens for the anxiety, OCD, or depression that so often travel with it.
Why it happens
The most-cited neuroscience comes from a 2017 study that scanned people with misophonia while they heard trigger sounds. Compared with controls, their brains showed greatly exaggerated activity in the anterior insular cortex — a hub for interoception and emotional salience — along with abnormal connectivity to the amygdala and prefrontal cortex, and increased heart rate and skin conductance during triggers [3]. In plain terms: the brain is tagging a specific, often harmless sound as urgent and threatening, and the body responds as if it were.
This is why misophonia feels involuntary and physical rather than chosen. It also reframes the goal of treatment: you are not trying to "decide" to stop caring about the sound, but to change how strongly your nervous system flags it and how much power the reaction holds over your next move. For a system that already processes sensory salience intensely — as in autism — that flag can be set lower and fire more easily, which fits what clinicians see [4]. Misophonia research is still young and its mechanisms are still being refined, so it is best understood as an actively studied condition rather than a settled one.
What actually helps
Evidence-based options
The most consistently studied treatment is cognitive behavioral therapy adapted for misophonia. In the first randomized controlled trial, a structured CBT protocol — combining attention and arousal-reduction strategies with changing the relationship to trigger sounds — produced meaningful clinical improvement in a substantial share of participants, with effects maintained at one-year follow-up [5]. A broader review of misophonia treatments reached a similar conclusion: CBT-based approaches currently have the strongest, though still emerging, evidence base [6].
For autistic adults, the principle is the same but the delivery should be tailored. That means accounting for your sensory profile (a technique that itself overwhelms you is counterproductive), respecting your communication preferences, and treating co-occurring anxiety or OCD in parallel rather than waiting. Practical coping tools — sound-shaping with low-level background noise, planned breaks, environmental design, and clear scripts for asking others to adjust — also genuinely help day to day, and there is a fuller set of misophonia coping strategies worth working through. Therapy and coping skills work best together rather than as separate tracks.
What to be cautious of
There is no medication approved specifically for misophonia, and claims of a quick "cure" should be treated skeptically — the realistic goal is reduced reaction intensity and better function, not erasing triggers. Pure avoidance, while understandable, tends to shrink your world over time and can strengthen the threat response rather than ease it. And approaches borrowed wholesale from tinnitus or hyperacusis care do not always transfer, because the mechanism differs. If a provider promises a fast fix, that is a reason to ask more questions, not fewer.
🔧 Key takeaway: Adapted CBT plus practical coping skills has the best current evidence; be wary of "cure" promises, and remember the realistic aim is a smaller, more manageable reaction.

When to get evaluated
Not every sound annoyance needs a clinician. A simple heuristic: if your reactions to specific sounds are intense, consistent, and shrinking your life — changing how you eat, work, or stay close to people — it is worth a formal look. If they are mild and occasional, coping strategies alone may be enough. And if sound sensitivity comes bundled with lifelong social, sensory, and routine differences you have never had assessed, consider a broader neurodevelopmental evaluation, not just a misophonia consult.
If you decide to pursue an assessment, here are concrete questions you can ask a provider:
Do you assess misophonia as its own pattern, or only as part of a general "sensory issues" label?
How will you tell misophonia apart from hyperacusis and from autistic sensory overload in my case?
Do you screen for co-occurring anxiety, OCD, and depression, and treat them alongside the sound reactions?
How do you adapt treatment for autistic adults — my sensory profile, communication style, and history of masking?
You can ask these directly when you reach out to us. The goal of the first conversation is not a label — it is a clear picture of what is happening and what would actually help.
🤝 Key takeaway: Seek an evaluation when sound reactions are intense, consistent, and narrowing your life — and bring questions that make sure the assessment looks at the whole picture.
Where this leaves you
Misophonia is real, it is more common in autistic adults than in the general population, and it is not a character flaw or a failure of patience. It is a sound-specific reaction with measurable roots in how the brain tags certain sounds — distinct from the broader sensory overload many autistic adults carry, and usually accompanied by anxiety, OCD, or depression worth addressing in its own right. None of that means you are stuck: the reaction can be understood, mapped, and softened.
If the patterns here feel familiar and they are wearing on your days, talking with a clinician who treats sound sensitivity as a real, specific thing — and who understands how it sits within an autistic nervous system — can help you build a plan that fits. Our team offers assessment and specialized therapy by telehealth across Tennessee, at a pace that respects how your system works.
Frequently Asked Questions
Is misophonia a sign of autism?
Not on its own. Misophonia — a strong, involuntary reaction to specific trigger sounds — occurs in autistic and non-autistic people alike. But research shows autistic traits and sensory sensitivities are elevated in people with misophonia, and it appears more often in autistic adults than in the general population. When sound sensitivity sits alongside lifelong social, sensory, and routine differences, an autism evaluation may be worth considering.
What's the difference between misophonia and autistic sensory overload?
Misophonia is triggered by specific sounds — often chewing, breathing, or tapping — and produces a fast, intense reaction even at low volume. Sensory overload builds from the cumulative load of many inputs at once, like noise, light, and crowds, until your system is overwhelmed. Misophonia is sound-specific and immediate; overload is additive and broad. Many autistic adults live with both.
Does misophonia get worse with anxiety or OCD?
It can feel that way. Roughly 79% of autistic people with misophonia also have a psychiatric condition such as anxiety, OCD, or depression, and higher stress tends to lower your threshold for trigger sounds. Treating co-occurring anxiety or OCD often makes misophonia more manageable, which is why a thorough assessment looks at the whole picture rather than the sound reactions alone.
Can therapy actually help misophonia?
Yes, for many people. Cognitive behavioral therapy is the most consistently studied approach, and a randomized trial found meaningful clinical improvement in a substantial share of participants, with gains holding at one-year follow-up. Therapy does not erase the triggers, but it can lower the intensity of the reaction and build coping tools. For autistic adults, the approach should be adapted to your sensory profile and communication style.
Does misophonia treatment work over telehealth?
Often, yes. Misophonia care relies on talk-based strategies — understanding your triggers, building coping skills, and addressing co-occurring anxiety or OCD — all of which translate well to video sessions. Telehealth can also be gentler on a sensitive nervous system, since you control your own environment. We offer assessment and therapy by telehealth across Tennessee.
About the Author
Dr. Kiesa Kelly is a licensed clinical psychologist and the founder of ScienceWorks Behavioral Healthcare, with more than 20 years of experience in psychological assessment and evidence-based treatment. Her work centers on adult neurodevelopmental evaluation — including autism and ADHD — and the sensory, emotional, and regulatory differences that come with them. She has particular interest in the conditions that are easy to miss in adults who have spent years masking and compensating.
Dr. Kelly's clinical training spans assessment of neurodevelopmental and co-occurring mental health conditions, and she leads a telehealth-forward practice serving Tennessee. Every article on this site is reviewed for clinical accuracy before publication.
References
1. Aldakhil A, et al. Misophonia in autism: A systematic review of prevalence, clinical features, and comorbidities. Research in Developmental Disabilities. 2025. https://pubmed.ncbi.nlm.nih.gov/40209614/
2. Swedo SE, Baguley DM, Denys D, et al. Consensus Definition of Misophonia: A Delphi Study. Frontiers in Neuroscience. 2022;16:841816. https://www.frontiersin.org/articles/10.3389/fnins.2022.841816/full
3. Kumar S, Tansley-Hancock O, Sedley W, et al. The Brain Basis for Misophonia. Current Biology. 2017;27(4):527-533. https://www.sciencedirect.com/science/article/pii/S0960982216315305
4. Rinaldi LJ, Simner J, Koursarou S, Ward J. Autistic traits, emotion regulation, and sensory sensitivities in children and adults with Misophonia. Journal of Autism and Developmental Disorders. 2023;53(3):1162-1174. https://link.springer.com/article/10.1007/s10803-022-05623-x
5. Jager IJ, Vulink NCC, Bergfeld IO, van Loon AJJM, Denys DAJP. Cognitive behavioral therapy for misophonia: A randomized clinical trial. Depression and Anxiety. 2021;38(7):708-718. https://onlinelibrary.wiley.com/doi/full/10.1002/da.23127
6. Mattson SA, et al. A systematic review of treatments for misophonia. Frontiers / NIH PMC. 2023. https://pmc.ncbi.nlm.nih.gov/articles/PMC10276561/
7. Brout JJ, Edelstein M, Erfanian M, et al. Investigating Misophonia: A Review of the Empirical Literature, Clinical Implications, and a Research Agenda. Frontiers in Neuroscience. 2018;12:36. https://www.frontiersin.org/articles/10.3389/fnins.2018.00036/full
8. National Institute for Health and Care Excellence (NICE). Autism spectrum disorder in adults: diagnosis and management (CG142). https://www.nice.org.uk/guidance/cg142
9. Ward J, et al. Misophonia symptoms in autistic adults (preprint; emerging evidence, not yet peer-reviewed). medRxiv. 2026. https://www.medrxiv.org/content/10.64898/2026.01.09.26343757v1.full
Disclaimer
This article is for informational purposes only and is not a substitute for professional medical or psychological advice, diagnosis, or treatment. Reading it does not create a clinician–patient relationship. If you are concerned about misophonia, autism, or any related condition, please consult a qualified healthcare provider. If you are in crisis or thinking about harming yourself, call or text 988 (the Suicide and Crisis Lifeline) in the United States.