
PHQ-9 vs. GAD-7 vs. PROMIS-29: How Three Common Screeners Answer Three Different Questions
- Kiesa Kelly

- 2 days ago
- 12 min read
Last reviewed: 04/24/2026
Reviewed by: Dr. Kiesa Kelly

If you have searched for a mental health questionnaire online, you have probably seen three names come up again and again: the PHQ-9, the GAD-7, and the PROMIS-29. They look similar at first glance — short, numbered items, a two-week time window, a score at the end. But they do not answer the same question. Pick the wrong one and you can walk away with a number that feels meaningful and still miss what is actually happening.
The PHQ-9 measures depression severity. The GAD-7 measures generalized anxiety severity. The PROMIS-29 measures seven different health domains at once, including depression and anxiety but also pain, fatigue, sleep, and function. Different questions, different uses, different thresholds.
In this article, you will learn:
What each screener actually measures, in plain language
When to reach for a single-symptom tool like the PHQ-9 or GAD-7 versus a multi-domain tool like the PROMIS-29
Score cutoffs for each instrument, side by side
What a high score does — and does not — mean clinically
What to do once you have a number in hand
The tension this post resolves: if you have ever stared at a list of questionnaires and thought "which one am I supposed to be taking," the answer is not "all of them" but "the one that matches the question you are trying to answer." If you want context on how these tools fit into a broader mental health screening process, that lives on a separate page.
What each screener actually measures
Let us start with the core purpose of each tool. This is answer-first: if you only read this section, you should already be able to pick correctly.
PHQ-9: depression severity in the last two weeks
The PHQ-9 is a nine-item depression screener developed from the PRIME-MD diagnostic instrument. Each item maps directly to one of the nine DSM criteria for major depressive disorder — low mood, loss of interest, sleep changes, appetite changes, fatigue, feelings of worthlessness, concentration problems, psychomotor changes, and thoughts of self-harm. You rate how often each symptom has bothered you over the past two weeks on a 0–3 scale, and the items sum to a 0–27 severity score.[1]
In the original validation study of more than 6,000 primary care and OB-GYN patients, Kroenke and colleagues found that a PHQ-9 score of 10 or higher identified major depression with 88% sensitivity and 88% specificity against a structured clinical interview.[1] That single cutoff is the reason this instrument became the default depression screener in American primary care. Recent meta-analyses continue to support a cutoff of 10 as the balanced threshold for screening, with individual patient-data analyses putting pooled sensitivity and specificity both around 0.85 at that threshold.[2]
The distinguishing pattern: the PHQ-9 answers "how severe is depression right now," item by DSM item, over the past two weeks. It is a depth gauge for one specific well.
GAD-7: generalized anxiety severity in the last two weeks
The GAD-7 is a seven-item anxiety screener built the same way. Spitzer, Kroenke, Williams, and Löwe developed it in 2006 by starting with a longer pool of DSM-based anxiety items and narrowing to the seven that best captured generalized anxiety disorder in a primary care sample of 2,740 adults.[3] Like the PHQ-9, you rate each item on 0–3 for the past two weeks, and the items sum to a 0–21 severity score.
In the original validation, a GAD-7 cutoff of 10 or higher produced 89% sensitivity and 82% specificity for GAD against a structured interview.[3] The instrument was designed for GAD specifically, but subsequent work has shown it performs reasonably well as a general anxiety screener, flagging panic disorder, social anxiety, and PTSD with moderate sensitivity — though it is not diagnostic for those conditions.[3] A 2023 systematic review and meta-analysis of GAD-7 performance across more than 40,000 participants confirmed that the cutoff of 10 continues to perform well for generalized anxiety detection, with pooled sensitivity around 0.83 and specificity around 0.84.[4]
The distinguishing pattern: the GAD-7 answers "how severe is generalized anxiety right now." Like the PHQ-9, it goes deep on one specific domain — worry, restlessness, irritability, and the physical tension that travels with them.
PROMIS-29: seven health domains at once
The PROMIS-29 is different in both shape and purpose. It is a 29-item profile from the NIH-funded Patient-Reported Outcomes Measurement Information System, designed to give a broad snapshot of health-related quality of life. It measures seven domains with four items each — physical function, anxiety, depression, fatigue, sleep disturbance, ability to participate in social roles, and pain interference — plus a single numeric rating for pain intensity.[5]
Unlike the PHQ-9 and GAD-7, PROMIS-29 does not use raw sums as the primary output. Each domain is scored on a T-score metric where 50 is the mean of the U.S. general population and 10 points equals one standard deviation. A depression T-score of 60 means you are one SD above the population average for depressive symptoms; a physical function T-score of 40 means one SD below average. Cella and colleagues validated the v2.0 profile in a U.S. general-population sample spanning ages 18 to 85 and showed that each domain held together psychometrically across age, gender, and chronic-condition subgroups.[5] More recent work has reinforced the measurement stability of these seven domains across clinical and general populations.[6]
The distinguishing pattern: the PROMIS-29 answers "how is your whole health landscape right now." It is a wide-angle lens, not a depth gauge. You give up some precision on any single domain in exchange for seeing how domains interact.
When to reach for which screener
Before the decision rules, a few misconceptions worth clearing up — because these are the traps that send people toward the wrong instrument.
"A higher score on any screener means I am sicker." Not exactly. Higher scores mean more symptom burden in whatever domain the screener actually measures. A PHQ-9 of 15 and a GAD-7 of 15 are not interchangeable — the first is moderately severe depression, the second is moderately severe anxiety, and they call for different next steps.
"Screeners diagnose conditions." They do not. Even at the best-studied cutoffs, the PHQ-9 and GAD-7 are sensitive and specific screeners, not diagnostic tools. A positive screen means a clinician should look more carefully, not that the diagnosis is confirmed.[1,3,7]
"If I take the PROMIS-29, I do not need the PHQ-9 or GAD-7." Sometimes true, often not. The PROMIS-29 gives you a good wide-angle read on depression and anxiety, but if either domain comes back elevated, you typically still want a domain-specific follow-up tool to track change over time. The PHQ-9 and GAD-7 have decades of treatment-response data behind their numbers; the PROMIS depression and anxiety short forms are newer in that role.
Now the decision.
Single-symptom check-in (PHQ-9 or GAD-7)
Reach for the PHQ-9 or GAD-7 when you have a specific symptom domain you want to measure precisely and track over time.
Consider someone who has been feeling flat for three weeks — cannot get excited about weekend plans, sleeping too much, losing interest in a hobby they usually love, finding themselves hollowed out by small inconveniences that used to bounce off them. They have noticed a creeping pull toward "nothing matters" thinking. This is a depression question. The PHQ-9 is the right tool because it maps one-to-one to DSM depression criteria, gives a defensible severity number, and has been validated for tracking treatment response over weeks and months.[1,2]
Or consider someone whose body has been loud for two weeks — tight chest in the mornings, jaw tension by afternoon, a running internal monologue about work emails and health symptoms and the kid's school situation, sleep fractured by 3 a.m. rumination. They are not sad; they are wired. This is an anxiety question. The GAD-7 is the right tool. It captures the cognitive and physical features of generalized anxiety — worry, restlessness, irritability, trouble relaxing — and gives a severity score you can retake in a month to see whether treatment is helping.[3,4]
Key takeaway: 🎯 If you can name the domain — "I think this is depression" or "I think this is anxiety" — pick the matching single-domain screener. You will get more useful numbers for tracking than you would from a broader tool.

Multi-domain self-check (PROMIS-29)
Reach for the PROMIS-29 when you do not know yet what domain you are dealing with — or when you suspect several domains are in play at once.
Consider someone recovering from a six-month medical problem that has cleared physically but left them diminished. They are tired more than the surgery alone can explain. They are not sure whether their flat mood is depression or deconditioning. Sleep is patchy. They avoid social events because they get worn out too fast. Is this depression? Fatigue? Pain? Some interaction of all three? The PROMIS-29 is built for exactly this question. It gives you T-scores across seven domains so you can see the shape of the problem, not just its name.[5,6]
Or consider someone going through a long-running family stressor who is noticing changes in sleep, energy, social withdrawal, low-grade pain, and irritability, but does not meet obvious full-threshold criteria for any one condition. The PROMIS-29 will show you which domains are most elevated relative to the general population and which are still in normal range. That pattern often matters more than any single number.
Key takeaway: 🗺️ Use the PROMIS-29 as a first-pass map. If two or three domains light up, you can then go domain-specific — PHQ-9 for depression, GAD-7 for anxiety, a sleep or pain tool for those specifically — to get more precise tracking.
Score ranges side by side
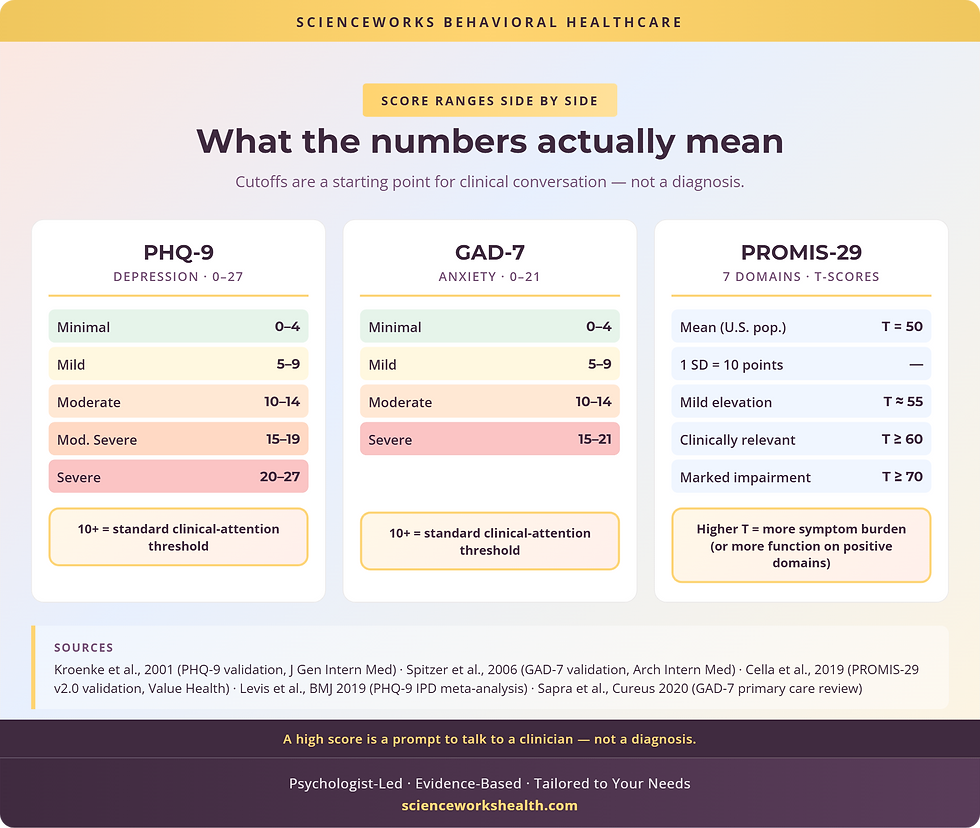
Here is where the numbers live. Keep in mind that screener cutoffs are starting points for clinical conversation, not diagnoses.
PHQ-9
Items: 9. Range: 0–27. Domain: Depression. Key cutoffs: 0–4 minimal; 5–9 mild; 10–14 moderate; 15–19 moderately severe; 20–27 severe. 10+ is the standard clinical-attention threshold.[1,2]
GAD-7
Items: 7. Range: 0–21. Domain: Generalized anxiety. Key cutoffs: 0–4 minimal; 5–9 mild; 10–14 moderate; 15–21 severe. 10+ is the standard clinical-attention threshold.[3,4]
PROMIS-29
Items: 29. Range: T-scores per domain. Domains: 7 — physical function, anxiety, depression, fatigue, sleep disturbance, social roles, pain interference (plus pain intensity 0–10). Anchors: Mean = 50, SD = 10. Higher T = more of the domain measured (more symptoms for negative domains, more function for positive ones). ~60+ on a symptom domain suggests meaningful elevation; ~40- on physical function / social roles suggests meaningful impairment.[5,6]
A decision heuristic you can apply right now:
If your question is specifically about depression → PHQ-9.
If your question is specifically about anxiety → GAD-7.
If you are not sure, or you suspect multiple domains are tangled up → PROMIS-29 first, then follow up with the PHQ-9 and/or GAD-7 if those domains are elevated.
Key takeaway: 📊 The PHQ-9 and GAD-7 share a 10+ clinical-attention cutoff on summed scores. The PROMIS-29 uses T-scores relative to the U.S. population mean of 50 — a different math, a different interpretation.
What a high score does and does not mean
A high PHQ-9, high GAD-7, or elevated PROMIS-29 domain is a signal, not a verdict. It tells you and a clinician that symptom burden is significant enough to warrant a closer look.[7,8] It does not tell you the cause (depression symptoms can come from a primary mood disorder, trauma, chronic pain, substance use, grief, or medication side effects — a number cannot sort these out), the right treatment (a PHQ-9 of 18 might respond best to therapy, to medication, to a combination, or to treating an underlying medical condition first), or whether you meet full diagnostic criteria (screeners are designed to be sensitive, so they sometimes flag people who do not ultimately meet full criteria, and the reverse can happen too).[1,3]
One important caveat on the PHQ-9: item 9 asks about thoughts of self-harm. Any non-zero response on that item, regardless of the total, warrants same-day clinical follow-up. If you are answering that item honestly and scoring above 0, please reach out to a crisis resource (988 in the U.S.) or a clinician today.
Key takeaway: 🚪 Screener scores are doors, not destinations. A number above cutoff says "it is worth looking," not "here is what you have."
What to do after you see your number
Once you have a score, there are roughly three scenarios.
Score below cutoff. If your symptoms are in the minimal range and that matches how you feel, retake in a few weeks if things change. If the low score feels wrong — some people under-report because they compare themselves to a worse moment, or because certain symptoms do not feel like "symptoms" to them — consider a broader tool like the PROMIS-29, or ask a clinician with formal psychological assessment training to help sort signal from noise.
Score above cutoff and feels accurate. A positive screen is a reasonable prompt to schedule a clinical evaluation. Bring the score with you. Most clinicians will do a fuller diagnostic interview, may repeat the screener or add others, and will talk through treatment options. In our practice, we often use the PHQ-9 or GAD-7 every few weeks during treatment to track whether the intervention is working.
Score above cutoff and the number surprises you. Sometimes people score higher than expected because they have normalized a level of symptom burden that is not actually normal — this is especially common with anxiety, where chronic tension can become the baseline. If anxiety or depression has been affecting daily life, a specialized therapy evaluation is a reasonable next step to clarify what is happening and what would help.
Key takeaway: 🧭 The score is the start of a plan, not the plan itself. Use it to decide whether and how to bring another person — ideally a clinician — into the picture.
FAQ
Is the PHQ-9 enough by itself?
For a first-pass depression check in primary care or self-monitoring, yes — it is one of the most thoroughly validated brief depression instruments in the literature.[1,2] It is not enough by itself for a formal diagnosis, and it is not enough by itself if anxiety, trauma, or another condition is the main driver. A positive PHQ-9 should be followed by a clinical interview, and if anxiety is also part of the picture, pairing with the GAD-7 is standard practice.[7]
Can I take the GAD-7 and PHQ-9 together?
Yes, and in fact this is how both instruments are most commonly used in integrated primary care — the so-called PHQ-9/GAD-7 combined screen.[7,8] Depression and anxiety co-occur often enough that measuring both at once gives a more complete picture than either alone. If you get elevated scores on both, the pattern is worth flagging to a clinician; combined depression-plus-anxiety presentations often benefit from treatment approaches that address both.
Is the PROMIS-29 a diagnosis?
No. None of these instruments provide a diagnosis. The PROMIS-29 is a profile of symptom burden and function across seven health domains, expressed in T-scores relative to the U.S. general population.[5,6] An elevated depression domain on the PROMIS-29 is a reason to look more closely at depression — potentially with the PHQ-9 and a clinical interview — not a diagnosis on its own. The same logic applies to every other domain on the profile.
Next step: take a screener and talk to a ScienceWorks clinician
If you have read this far, you probably have a better sense of which instrument fits your question. The honest next step is to take the one that matches and then do something with the result.
If your question is specifically about depression, the PHQ-9 is available as a free tool you can take in a few minutes.
If the question is about anxiety, do the GAD-7 instead.
If you are not sure, start with the PROMIS-29 and let the elevated domains tell you where to look next.
Whatever score comes back, it is information — not a label. If you would like a clinician to help you interpret what your results mean and decide what to do next, we are happy to have that conversation. You can reach out to schedule an evaluation and bring your scores with you. We do this work every day, and a number with a thoughtful conversation around it is much more useful than a number alone.
About the Author
Dr. Kiesa Kelly is a licensed clinical psychologist and the founder of ScienceWorks Behavioral Healthcare. Dr. Kelly has more than 20 years of experience in psychological assessment and evidence-based treatment for adults and adolescents, including diagnostic evaluations for depression, anxiety, ADHD, autism, trauma, OCD, and sleep disorders.
Her clinical practice emphasizes measurement-based care — using validated instruments like the PHQ-9, GAD-7, and PROMIS-29 to guide treatment decisions and track progress over time. Every blog post on scienceworkshealth.com is reviewed by Dr. Kelly for clinical accuracy before publication.
References
1. Kroenke K, Spitzer RL, Williams JBW. The PHQ-9: Validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1495268/
2. Levis B, Benedetti A, Thombs BD, et al. Accuracy of Patient Health Questionnaire-9 (PHQ-9) for screening to detect major depression: individual participant data meta-analysis. BMJ. 2019;365:l1476. https://www.bmj.com/content/365/bmj.l1476
3. Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/410326
4. Sapra A, Bhandari P, Sharma S, Chanpura T, Lopp L. Using generalized anxiety disorder-2 (GAD-2) and GAD-7 in a primary care setting. Cureus. 2020;12(5):e8224. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7292717/
5. Cella D, Choi SW, Condon DM, et al. PROMIS® adult health profiles: efficient short-form measures of seven health domains. Value Health. 2019;22(5):537–544. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6512855/
6. Hanmer J, Jensen RE, Rothrock N; HealthMeasures Team. A reporting checklist for HealthMeasures' patient-reported outcomes: ASCQ-Me, Neuro-QoL, NIH Toolbox, and PROMIS. J Patient Rep Outcomes. 2020;4(1):21. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7067945/
7. US Preventive Services Task Force. Screening for depression and suicide risk in adults: US Preventive Services Task Force recommendation statement. JAMA. 2023;329(23):2057–2067. https://jamanetwork.com/journals/jama/fullarticle/2805707
8. US Preventive Services Task Force. Screening for anxiety disorders in adults: US Preventive Services Task Force recommendation statement. JAMA. 2023;329(24):2163–2170. https://jamanetwork.com/journals/jama/fullarticle/2805704
9. American Psychiatric Association. Practice guideline for the treatment of patients with major depressive disorder, third edition. Arlington, VA: APA Publishing; 2010. https://psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/guidelines/mdd.pdf
10. National Institute of Mental Health. Major depression statistics. Bethesda, MD: NIMH; 2023. https://www.nimh.nih.gov/health/statistics/major-depression
11. National Institute of Mental Health. Any anxiety disorder statistics. Bethesda, MD: NIMH; 2023. https://www.nimh.nih.gov/health/statistics/any-anxiety-disorder
12. Negeri ZF, Levis B, Sun Y, et al. Accuracy of the Patient Health Questionnaire-9 for screening to detect major depression: updated systematic review and individual participant data meta-analysis. BMJ. 2021;375:n2183. https://www.bmj.com/content/375/bmj.n2183
Disclaimer
The information in this article is provided for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Screener scores do not diagnose any condition. If you are experiencing a mental health concern, please consult with a qualified licensed clinician. If you are in crisis or having thoughts of self-harm, call or text 988 (the Suicide and Crisis Lifeline) or go to your nearest emergency department.

