
"I Saw Myself in My Child's Diagnosis": Recognizing Your Own Autism or ADHD After Your Kid Is Evaluated
- Kiesa Kelly

- Jun 3
- 14 min read
Last reviewed: 06/03/2026
Reviewed by: Dr. Kiesa Kelly
You sat through your child's evaluation, read the report, and somewhere in the descriptions of how they think, focus, or move through the world, you felt a quiet jolt of recognition. Wait — that's me, too. If that's where you are right now, you're not imagining things, and you're not alone. Recognizing your own ADHD or autism after your child is diagnosed is one of the most common doorways adults walk through on their way to understanding their own neurodivergence.
It makes sense once you see the genetics. Both conditions are highly heritable, so a child's diagnosis routinely shines a light on a parent who was never identified. This article is for the parent who is suddenly asking, "Is this me too?" — and wants to know what to do with that question.
In this article, you'll learn:
Why a child's evaluation so often reveals a parent's own neurodivergence
The traits parents most commonly recognize in themselves
How to make sense of grief, relief, and the tangle of feelings that follow
Whether an adult diagnosis actually changes anything (it can)
How adult ADHD and autism evaluation works, including the childhood-records question
How to support your child and yourself at the same time
Short answer: recognizing yourself in your child's diagnosis is common, and it's worth taking seriously
Here's the short version. Seeing yourself in your child's autism or ADHD profile is a genuine, well-recognized pathway to adult identification — and it's worth following up on rather than waving away. It isn't a coincidence, and it isn't you over-identifying with your kid. Both conditions are strongly genetic, so a parent who quietly struggled for decades often only gets language for it when a clinician spells out the same pattern in their child.
Recognition is a strong starting signal, but it is not a diagnosis on its own. The next step, if you want clarity, is an adult assessment that accounts for how these conditions show up after years of masking and compensation. Many parents tell us the recognition feels both disorienting and, eventually, like a relief — finally there's a frame that fits.
One thing to set down right away: noticing this about yourself does not make you a worse parent. If anything, parents who understand their own wiring often become more patient and more attuned to what their child actually needs.
🧩 Key takeaway: Seeing yourself in your child's diagnosis is a recognized route into adult identification — common, valid, and worth a closer look, not a reason for self-doubt.

Why a child's evaluation so often reveals a parent's neurodivergence (the genetics)
The reason this happens so reliably comes down to heritability — how much of the variation in a trait across a population is explained by genetic differences. Both ADHD and autism are among the most heritable conditions in psychiatry. Large twin and family studies estimate ADHD heritability at roughly 70 to 80 percent [1][2], and autism heritability in a similar high range, with estimates clustering between about 60 and 90 percent depending on the sample and method [3][4]. In plain terms: if a child has ADHD or autism, there is a meaningfully elevated chance that a biological parent shares some of the same neurodevelopmental wiring.
That's why a pediatric or psychological assessment can feel like a mirror held up to the whole family. The clinician describes your child's difficulty with transitions, their need for routine, their attention that scatters under boredom but locks in under interest — and you realize you've lived inside that description your entire life. You weren't looking for a diagnosis. You were reading about your kid. And there you were on the page.
Let's clear up a few misconceptions that keep parents stuck right here.
"If I really had it, someone would have caught it when I was a kid." Not necessarily. Diagnostic criteria, awareness, and access have all shifted dramatically over the past few decades. Many adults — especially women and people who learned to mask early — moved through childhood without anyone connecting the dots, because the older picture of ADHD and autism was narrow and male-coded [5]. Being missed as a child is the norm for late-identified adults, not the exception. If you're a parent recognizing this in midlife, our deep dive on late-identified autism after 40 speaks directly to how often these traits surface only later in life.
"My child's diagnosis means I passed something bad on to them." This is the belief that hurts the most, and it's the one that's most worth correcting. Heritability is not blame. Sharing neurodevelopmental wiring with your child isn't a failure or a defect you transmitted — it's simply how genetics work across a family. Neurodivergence is a difference in brain wiring, not damage. We'll come back to this, because the feeling behind it deserves more than a single line.
"I'm just over-identifying because I'm emotionally involved." It's reasonable to wonder. But recognition that's rooted in genuine lifelong patterns — not a passing "oh, I do that too" — is exactly the kind of signal clinicians take seriously. A structured evaluation is precisely the tool that tells the difference between real shared traits and understandable parental projection.
🧬 Key takeaway: ADHD and autism are highly heritable, so a child's diagnosis statistically raises the odds a parent shares the wiring — recognition is the genetics surfacing, not a fluke.
The traits parents most often suddenly recognize
When the recognition lands, it usually isn't a single dramatic symptom. It's a cascade of small, lifelong things you'd long since filed under "just how I am." Here are the patterns parents most often describe to us.
"I just thought everyone struggled with this"
This is the phrase we hear most. So much of undiagnosed neurodivergence hides behind the assumption that everyone finds these things equally hard — and that you're simply worse at coping.
Picture the parent who has spent thirty years believing everyone has to write themselves four reminders to send one email, re-reads the same paragraph three times because their attention slid off the page, and feels genuinely drained after a birthday party that everyone else seemed to enjoy. They assumed this was universal, that other people just powered through better. Reading their child's ADHD report, they see "difficulty sustaining attention on non-preferred tasks" and "executive functioning challenges" described as clinical features — not personal failings — and something reorganizes inside them.
Or picture the parent at their child's autism evaluation who hears the clinician describe sensory sensitivity, a need for predictability, and the exhaustion of unstructured social time. They've spent a lifetime quietly engineering their environment — same coffee shop, same seat, headphones always within reach — and calling it "being particular." Hearing it named as a recognized neurodevelopmental pattern, rather than a quirk to apologize for, is the moment the floor shifts. They weren't high-maintenance. They were managing a nervous system nobody had ever explained to them.
The lifetime of compensations that finally have a name
The other big recognition is seeing your coping strategies for what they really are: compensations. Late-identified adults are often very good at hiding the struggle — that's why they were missed. The strategies were so effective, and so automatic, that they looked like personality instead of effort.
Think about the parent who is known as hyper-organized — color-coded calendars, alarms for everything, lists upon lists. From the outside it reads as type-A competence. From the inside, it's a scaffolding built brick by brick over decades because without it, everything falls apart. That's not natural orderliness; that's an exhausting external system propping up an executive-function difficulty. When their child gets an ADHD diagnosis and a clinician explains why these scaffolds help, the parent finally understands they've been compensating, not coasting.
Or consider the social compensation many late-identified autistic adults describe as camouflaging or masking — rehearsing conversations in advance, copying other people's expressions, monitoring their own tone in real time, and collapsing in private afterward. Research has linked this kind of sustained masking to real mental-health costs, including anxiety, depression, and burnout [6][7]. If you've spent your life performing "normal" and crashing after, and you're only now learning there's a name for it, that recognition can be both painful and validating in the same breath. A burnout pattern like this is worth understanding on its own; some adults find an autistic-burnout screener a useful first way to put language to it.
📋 Key takeaway: The coping strategies that made you look fine — the lists, the rehearsals, the rigid routines — are often the very compensations that hid your neurodivergence in plain sight.
Grief, relief, and the complicated feelings of a late recognition
Almost no one feels just one thing when this clicks into place. The emotional arc of late recognition is genuinely complicated, and it helps to expect that going in.
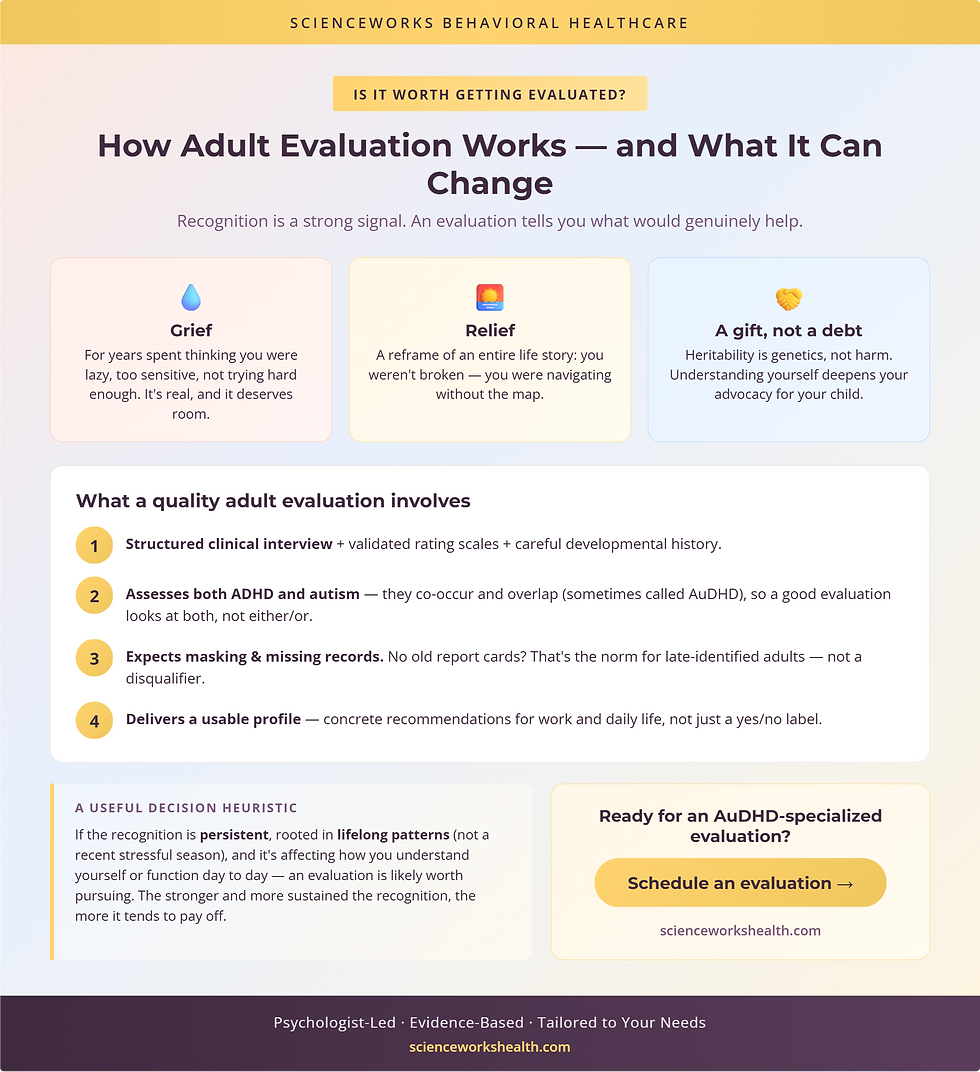
There is often grief. Grief for the years you spent thinking you were lazy, too sensitive, not trying hard enough. Grief for the support you never got, the accommodations no one offered, the version of your life that might have looked different if someone had understood you sooner. That grief is real and it deserves room. You're allowed to feel sad about it, even while you're grateful to understand yourself now.
There is also, very often, relief. A reframe of an entire life story. The realization that you weren't broken or failing — you were navigating the world with a brain that works differently, without the map. Many adults describe a profound softening of self-judgment once they have the language. The internal voice that said "what's wrong with you" finally has an answer that isn't an indictment.
And then there's the tender, complicated layer of feelings about your child. Some parents feel a pang of "did I do this to them?" — which circles back to the heritability point. Let's be clear and gentle about it: you did not fail your child by sharing genetics with them. Neurodivergence is not a wound you inflicted. In fact, many parents find that recognizing themselves becomes one of the most useful things they bring to their child's life — they understand the inside of the experience in a way few parents can.
🌡️ Key takeaway: Grief and relief usually arrive together. Both are valid. And the guilt about heritability eases when you remember that shared wiring is genetics, not harm — your understanding is a gift to your child, not a debt.
Does an adult diagnosis actually change anything? (yes — and how)
A fair question to ask before you spend time and money on an evaluation: does a diagnosis in adulthood actually do anything, or is it just a label? For many adults, it changes several concrete things.
Self-understanding and self-compassion. This is the change most adults name first. Research on late-identified adults — particularly late-diagnosed autistic adults — consistently finds that diagnosis is associated with relief, improved self-concept, and a more compassionate reinterpretation of past struggles [8][9]. Reframing decades of "I should have been able to do this" into "this was genuinely harder for my brain" is not a small thing.
Access to accommodations and support. A formal diagnosis can open doors that self-recognition alone can't: workplace accommodations, academic support if you're studying, and a clearer case for the adjustments that help you function. You can't always advocate for what you don't have a name for.
Treatment and strategy that actually fit. When you know what you're working with, support gets targeted. ADHD-informed coaching, autism-affirming therapy, and strategies built for your specific profile tend to land better than generic advice to "just try harder" or "be more organized."
A useful decision heuristic: if the recognition is persistent (not a passing thought), rooted in lifelong patterns rather than a recent stressful season, and it's affecting how you understand yourself or function day to day, an evaluation is likely worth pursuing. If it's a fleeting "huh, interesting" with no real impact, you can sit with it. The stronger and more sustained the recognition, the more an evaluation tends to pay off.
⚖️ Key takeaway: An adult diagnosis isn't just a label — for many people it changes self-understanding, unlocks accommodations, and makes support specific enough to actually help.
How adult ADHD/autism evaluation works (and the childhood-records question)
If you decide to pursue clarity, here's what a quality adult evaluation involves — and how clinicians handle the obstacles that worry parents most.
A thorough adult ADHD and autism assessment typically combines a structured clinical interview, validated rating scales, and a careful developmental history. Because both conditions can co-occur — and because the traits overlap — a good evaluation looks at both rather than forcing an either/or. When ADHD and autism show up together, the combined picture (sometimes called AuDHD) has its own texture; our explainer on how ADHD and autism overlap in adults is a useful companion if both feel true for you. The point isn't just a yes-or-no label; it's a clear picture of your profile and concrete recommendations you can use.
The question we hear most from parents is about childhood records. "I don't have my old report cards or anyone who remembers me as a kid — can I even be assessed?" The short answer is yes. A skilled clinician gathers developmental history through structured interview and your own recollections, and adapts when school files or childhood informants aren't available. Missing records are the norm for late-identified adults, not a disqualifier. (We cover this in depth in our guide on whether you need childhood records for an adult ADHD or autism diagnosis — worth a read if that's your main worry.)
Before you book anything, it helps to know what to ask. Here are concrete questions you can put to any provider:
Scope: "Does your evaluation assess for both ADHD and autism if both seem plausible, or only one?"
Methodology: "How does your process account for masking and lifelong compensation in adults who learned to hide their traits?"
Developmental history: "What developmental history do you gather if I don't have childhood records or someone who knew me as a child?"
Dual-diagnosis capability: "If both conditions are present, can you diagnose both, or would I need a separate referral for the second?"
Output: "What do I actually receive at the end — a diagnostic label only, or specific, usable recommendations for work, daily life, and any treatment?"
A few validated screeners can also help you organize your thinking before an evaluation. The ASRS is a widely used adult ADHD self-report screener [10], and the AQ-10 is a brief autism screener [11]. Neither diagnoses anything on its own — they're starting points, not endpoints. If your screening results raise more questions than they answer, that's exactly what a full evaluation is for; our mental-health screening page is a place to begin.
🔎 Key takeaway: A good adult evaluation assesses both conditions, expects masking, and works around missing childhood records — so don't let a lack of old paperwork talk you out of getting answers.
Supporting your child and yourself at the same time
A worry surfaces for a lot of parents here: if I turn attention toward myself, am I taking something away from my child? The honest answer is no — and often the opposite is true.
Understanding your own neurodivergence frequently makes you a more effective advocate, not a distracted one. When you know from the inside what sensory overload feels like, or why a transition is so hard, or what masking costs by the end of the day, you can translate for your child in ways other parents can't. Your recognition becomes a tool you bring to their corner.
Practically, your own evaluation doesn't have to compete with your child's care. There's no rule that says you must do both at once or in any particular order. Some parents pursue their own assessment soon after their child's, while the recognition is fresh and the motivation is high. Others wait until their child's supports are settled and their own bandwidth opens up. Both are reasonable. What isn't reasonable is the idea that your needs don't count — they do.
And modeling matters. A child who watches a parent take their own brain seriously, seek understanding without shame, and build supports that fit is learning something powerful about self-knowledge and self-respect. You're not subtracting from your child by understanding yourself. You're showing them how it's done.
🤝 Key takeaway: Understanding yourself doesn't compete with supporting your child — it usually deepens your advocacy, and it models the self-knowledge you want them to grow into.
We know this is a lot to hold — a new lens on your own life arriving in the middle of caring for your child's. You don't have to sort it out alone, and you don't have to have it figured out before you reach out.
Ready for an AuDHD-specialized evaluation?
If the patterns above feel familiar, an evaluation that looks at autism and ADHD together — not one or the other in isolation — can help name what's actually driving the overload.
Next step — see whether an adult evaluation is right for you
If reading your child's diagnosis turned a light on for you, that recognition deserves a real answer rather than a question you carry around. You've spent long enough wondering whether the way you move through the world has a name. An evaluation that looks at autism and ADHD together — and that expects the masking and missing records so common in adults — can tell you what's actually going on and, more importantly, what would help. Whether you decide to pursue it now or later, your needs are worth taking as seriously as your child's.
Frequently Asked Questions
I recognized myself in my child's diagnosis — does that mean I'm autistic or have ADHD too?
It's a meaningful signal worth taking seriously, but recognition is not a diagnosis. Both autism and ADHD run strongly in families, so a child's evaluation often surfaces traits a parent has carried for years. The way to find out is an adult evaluation that accounts for masking and lifelong compensation. Self-recognition is a reasonable starting point — not the answer by itself.
Did I cause or pass my ADHD or autism to my child?
Heritability is not fault. Both conditions are highly heritable — twin and family studies estimate ADHD heritability around 70–80% and autism around 60–90% — which means shared neurodevelopment, not something you did wrong. Neurodivergence isn't a defect passed down; it's a difference in how a brain is wired. Many parents find that understanding their own profile helps them parent with more compassion, not less.
Do I need my childhood records to get evaluated for ADHD or autism as an adult?
Usually not as a strict requirement. A skilled clinician can gather developmental history through structured interview, your own recollections, and sometimes input from family — masking and missing records are expected in late-identified adults. If you want to know exactly what stands in for a school file, our companion guide on whether you need childhood records for an adult diagnosis walks through it.
Is it worth getting an adult diagnosis if I've coped this long?
For many adults, yes. A diagnosis can reframe a lifetime of self-blame, open access to accommodations at work, guide treatment that actually fits, and improve self-understanding. Research on late-identified adults links diagnosis to relief and better self-concept for many. You've coped — but coping and thriving aren't the same, and an evaluation tells you what would genuinely help.
Should I get evaluated at the same time as my child or wait?
There's no single right order — it depends on your bandwidth. Some parents pursue their own evaluation soon after their child's because the recognition is fresh and motivating; others wait until their child's support is settled. What matters is that your needs are real and worth attention too. Supporting your child and understanding yourself aren't competing priorities.
About the Author
Dr. Kiesa Kelly is a licensed clinical psychologist and the founder of ScienceWorks Behavioral Healthcare, with more than 20 years of experience in psychological assessment and evidence-based treatment. Her work centers on neurodevelopmental evaluation across the lifespan, including adult ADHD and autism assessment — with particular attention to the late-identified adults and women whose traits were missed under older, narrower diagnostic pictures. Her clinical training spans major universities and assessment-focused settings, and she has long worked at the intersection of careful diagnosis and practical, affirming recommendations.
Dr. Kelly built ScienceWorks around the conviction that a good evaluation should leave a person with more self-understanding, not just a label. She brings that lens to families in particular, where a child's diagnosis so often opens a parent's own questions — and where holding both generations' needs with care is the work itself.
References
1. Faraone SV, Larsson H. Genetics of attention deficit hyperactivity disorder. Molecular Psychiatry. 2019;24(4):562–575. https://doi.org/10.1038/s41380-018-0070-0
2. Faraone SV, Banaschewski T, Coghill D, et al. The World Federation of ADHD International Consensus Statement: 208 evidence-based conclusions about the disorder. Neuroscience & Biobehavioral Reviews. 2021;128:789–818. https://doi.org/10.1016/j.neubiorev.2021.01.022
3. Tick B, Bolton P, Happé F, Rutter M, Rijsdijk F. Heritability of autism spectrum disorders: a meta-analysis of twin studies. Journal of Child Psychology and Psychiatry. 2016;57(5):585–595. https://doi.org/10.1111/jcpp.12499
4. Bai D, Yip BHK, Windham GC, et al. Association of genetic and environmental factors with autism in a 5-country cohort. JAMA Psychiatry. 2019;76(10):1035–1043. https://doi.org/10.1001/jamapsychiatry.2019.1411
5. Gould J. Towards understanding the under-recognition of girls and women on the autism spectrum. Autism. 2017;21(6):703–705. https://doi.org/10.1177/1362361317706174
6. Hull L, Petrides KV, Allison C, et al. "Putting on my best normal": social camouflaging in adults with autism spectrum conditions. Journal of Autism and Developmental Disorders. 2017;47(8):2519–2534. https://doi.org/10.1007/s10803-017-3166-5
7. Cassidy S, Bradley L, Shaw R, Baron-Cohen S. Risk markers for suicidality in autistic adults. Molecular Autism. 2018;9:42. https://doi.org/10.1186/s13229-018-0226-4
8. Stagg SD, Belcher H. Living with autism without knowing: receiving a diagnosis in later life. Health Psychology and Behavioral Medicine. 2019;7(1):348–361. https://doi.org/10.1080/21642850.2019.1684920
9. Huang Y, Arnold SR, Foley KR, Trollor JN. Diagnosis of autism in adulthood: a scoping review. Autism. 2020;24(6):1311–1327. https://doi.org/10.1177/1362361320903128
10. Kessler RC, Adler L, Ames M, et al. The World Health Organization Adult ADHD Self-Report Scale (ASRS): a short screening scale for use in the general population. Psychological Medicine. 2005;35(2):245–256. https://doi.org/10.1017/S0033291704002892
11. Allison C, Auyeung B, Baron-Cohen S. Toward brief "red flags" for autism screening: the Short Autism Spectrum Quotient and the Short Quantitative Checklist (AQ-10). Journal of the American Academy of Child & Adolescent Psychiatry. 2012;51(2):202–212. https://doi.org/10.1016/j.jaac.2011.11.003
12. National Institute for Health and Care Excellence (NICE). Autism spectrum disorder in adults: diagnosis and management (CG142). 2021. https://www.nice.org.uk/guidance/cg142
13. National Institute for Health and Care Excellence (NICE). Attention deficit hyperactivity disorder: diagnosis and management (NG87). 2019. https://www.nice.org.uk/guidance/ng87
Disclaimer
This article is for informational and educational purposes only and is not a substitute for professional medical or psychological advice, diagnosis, or treatment. Reading it does not crea