
EMDR for OCD: Does It Help, and When It Complements ERP
- Kiesa Kelly

- Apr 22
- 14 min read
Updated: Jul 15
Last reviewed: 04/21/2026
Reviewed by: Dr. Kiesa Kelly

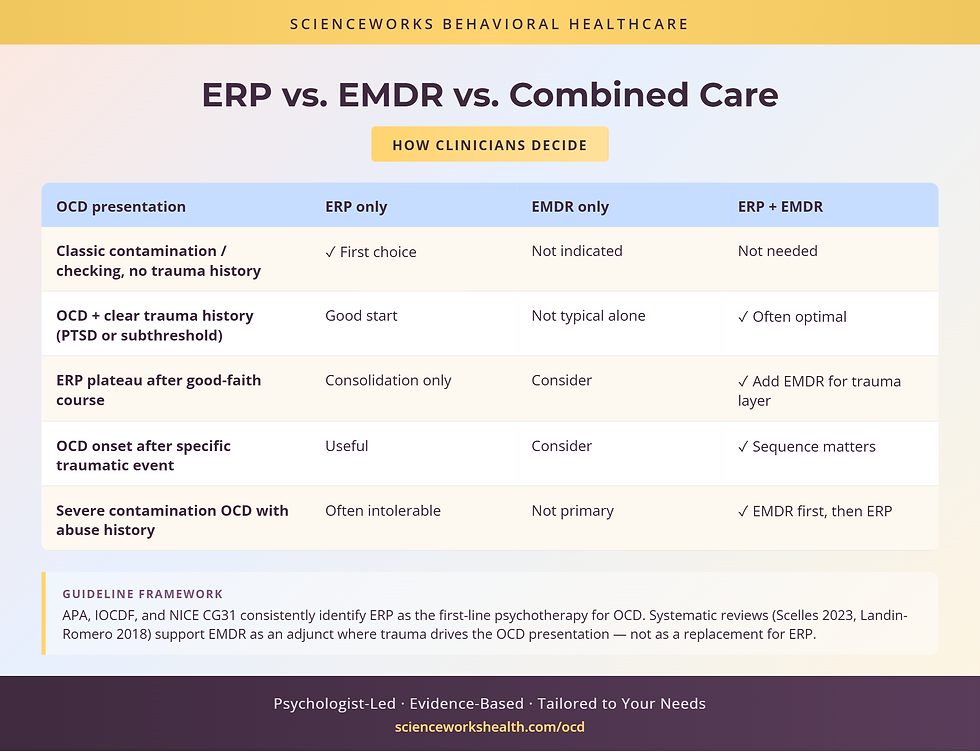
If you have been in OCD treatment — or researching it seriously — you have probably run into a question that the field itself is still working out: should EMDR be part of your care, or is ERP enough on its own? The short version, and the one most competent OCD clinicians will tell you, is that Exposure and Response Prevention remains the first-line psychological treatment for OCD, full stop. The longer, more useful version is that a subset of OCD presentations — particularly cases where early-life trauma or later traumatic experiences are clearly wound into the obsessive content — often benefit from adding EMDR alongside or adjacent to ERP. Knowing which subset you belong to is most of the decision.
In this article, you'll learn:
Why ERP is still considered the gold standard for OCD and where its limits sit
When a trauma-informed lens changes what OCD treatment should look like
What the current research says about EMDR for OCD — monotherapy, adjunct, and against medication
Specific OCD subtypes where EMDR-as-adjunct is most often considered
How to benchmark severity with the OCD symptom screener and use it to track progress
Concrete questions to ask a clinician about whether EMDR should be added to your plan
A note on framing: this post is about when and how to combine two evidence-based approaches — not about replacing one with the other. We do not treat EMDR as a substitute for ERP, and neither does any credible clinical body writing about OCD today.
Is EMDR an evidence-based treatment for OCD?
The short answer is: EMDR has a growing evidence base in OCD, but it is not positioned as a first-line monotherapy for OCD in any major clinical practice guideline. The International OCD Foundation, the American Psychiatric Association, and NICE all continue to identify ERP — often paired with a serotonergic medication for moderate-to-severe cases — as the first-line psychological treatment for OCD [1][2][3]. EMDR appears in the literature primarily in three contexts: as an adjunct to ERP for trauma-origin OCD, as a monotherapy in smaller controlled trials with mixed but generally promising results, and in treatment programs for comorbid OCD-PTSD presentations [4][5][6].
Misconception: If EMDR helps with OCD, it must work the same way ERP works. In reality, the two approaches target different mechanisms. ERP directly targets the obsession-compulsion cycle through exposure and response prevention — the reader systematically encounters their feared content without performing the compulsion, which allows the anxiety curve to drop on its own. EMDR targets the memory networks where distressing content is stored, and is most useful when a memory or set of memories appears to be feeding the obsessional content. The two are not interchangeable; they are operating on different levels of the system.
Key takeaway: 🧭 ERP is first-line for OCD and should not be skipped in favor of EMDR. EMDR earns its place in the plan when a trauma link to the OCD content is identifiable.
Why ERP is still the gold standard for OCD
The core mechanism of ERP
ERP works by confronting the obsessional trigger and preventing the compulsive response long enough for the brain to learn that the feared outcome does not follow — what the field now often describes as inhibitory learning, an update to the older habituation model [7]. Over enough repetitions, the association between the trigger and the anxiety response weakens, and the compulsion loses the reinforcement that sustains it. This is a direct, mechanistic intervention on the cycle itself, and it has been studied in thousands of participants across decades.
Where ERP alone can plateau
That said, experienced OCD clinicians recognize a subset of cases where ERP stalls despite competent delivery and good client engagement. Consider a person in their late twenties who has done eighteen months of high-quality ERP for contamination OCD. Their Y-BOCS score has dropped from the severe range into the moderate range, but it will not move further. Their compulsions have decreased, but the background distress around contamination triggers remains intense, and a particular memory from childhood — a medical procedure that was poorly handled — keeps surfacing in the ERP sessions themselves. For this person, the plateau is not a failure of ERP; it is a signal that the content being triggered has a memory-network component that exposure alone may not be reaching.
Or: a client in their forties with well-established harm-themed intrusive thoughts has done a full course of ERP, scripts and imaginal exposures included. The intrusive content no longer drives hours of compulsive checking — but the client still holds a deep, quiet belief that they are dangerous to the people they love. That belief, when probed carefully, ties to a specific traumatic event in early adolescence. The target for the remaining clinical work is not the intrusion; it is the adolescent memory.
The distinguishing pattern: ERP-responsive OCD is driven by the cycle itself — the behavior of the compulsion is sustaining the anxiety. Trauma-linked OCD layers a memory-network component on top, and addressing only the cycle can leave the memory network intact.
When a trauma-informed lens matters for OCD
There is a well-documented relationship between early-life adversity, traumatic experience, and OCD onset and severity [8]. Research consistently shows that a meaningful proportion of people with OCD also meet criteria for PTSD at some point, with co-occurrence estimates across adult samples ranging from roughly 19 to 41 percent depending on the population [9]. Childhood adversity exposure is elevated in OCD samples compared to non-clinical samples, and the relationship appears to be bidirectional: trauma can precipitate or intensify OCD, and OCD can magnify the distress of traumatic memory [8].
Early-life adversity and OCD onset
When the OCD onset in a given client tracks closely to a traumatic event or a period of chronic developmental adversity, the clinical formulation changes. The obsessional content often carries traces of the trauma — contamination fears after medical abuse, harm themes after exposure to violence, scrupulosity after religious coercion. In these cases, leaving the underlying memory network untouched and treating only the surface cycle can produce real but incomplete gains.
PTSD + OCD comorbidity
When full PTSD criteria are met alongside OCD, treatment planning is more complex. Both conditions have evidence-based treatments, both sets of treatments are demanding, and sequencing matters. In the literature, there is active discussion about whether to stabilize trauma first, treat OCD first, or work concurrently, and current practice generally tailors this to symptom severity, functional impairment, and client preference [5][6].
The subset where "stuck points" are trauma-origin
Not every client with a trauma history belongs in this subset. Many people with childhood adversity respond excellently to ERP alone, and adding trauma-focused work when it is not needed can slow treatment. The subset we are identifying is narrower: clients for whom specific obsessional content is anchored to a specific memory, clients whose ERP has plateaued in the way described above, or clients whose distress between ERP sessions spikes around a specific past event.
Misconception: A trauma history automatically means EMDR should be part of OCD treatment. In reality, having experienced trauma and having OCD content that is driven by that trauma are two different clinical findings. Many clients with significant trauma histories respond beautifully to ERP alone, and treatment planning should be driven by how the OCD content is organized, not by whether trauma is present somewhere in the life history.
Key takeaway: 🧩 A trauma-informed lens on OCD does not mean every OCD client needs EMDR. It means recognizing the subset where specific memories are feeding the obsessional content.
What the research shows for EMDR in OCD
EMDR-plus-ERP combined outcomes
Small-to-moderate-sized studies and clinical series of combined EMDR-plus-ERP protocols have generally reported additive benefits over ERP alone in trauma-comorbid OCD, particularly on distress ratings tied to the obsessional content and on quality-of-life measures [4][5]. The evidence base is not yet large enough to position combined treatment as a default, but it is large enough that the approach is reasonable and defensible when the clinical picture warrants it.
EMDR monotherapy findings and their limits
Controlled trials of EMDR as a standalone treatment for OCD — without ERP — have produced mixed results [4][10]. Some trials report Y-BOCS reductions comparable to, or in some samples slightly better than, a serotonergic medication condition. Other trials show more modest effects. Given that ERP has much stronger and more replicated evidence, and given that EMDR monotherapy studies vary in methodology, treatment dose, and population, the field has not moved toward EMDR-only OCD treatment as standard practice.
How EMDR performs against SSRI-only treatment
Where EMDR has been directly compared to SSRI-only conditions in OCD trials, it has generally performed at least as well as the medication condition on Y-BOCS endpoints, with differences in side effect burden and durability of effect [10]. This is a narrower finding than "EMDR is a general OCD treatment" — it speaks primarily to clients who cannot or prefer not to take medication — but it is relevant for clinicians and clients considering treatment options.
Misconception: EMDR is faster than ERP, so adding it should shorten OCD treatment. In reality, the opposite is often true. Adding a second evidence-based modality typically extends total treatment length, not shortens it, because each modality has its own arc and pacing. The reason to add EMDR is clinical fit, not time savings, and clients who are told the opposite should read that as a warning sign about the treatment plan.
The distinguishing pattern: The research supporting EMDR in OCD is strongest when EMDR is added to ERP or used in clients with clear trauma-OCD comorbidity, and weakest when EMDR is proposed as a substitute for ERP. Read evidence claims through that lens.
Key takeaway: 📊 EMDR-plus-ERP has meaningful evidence for trauma-linked OCD. EMDR as a standalone OCD treatment is supported by a smaller, less consistent literature.
How clinicians decide whether to add EMDR
The decision to add EMDR to an OCD treatment plan is rarely made at intake. It is usually made after enough ERP has been done to understand how the client's specific presentation responds, and whether there is content the ERP is not reaching.
Signs that trauma is driving the OCD presentation
When we consider adding EMDR for a client already in OCD care, we are looking for a few patterns together:
The OCD onset coincided with or closely followed a traumatic event
Specific obsessional content tracks thematically to a specific memory the client can identify
Distress between ERP sessions spikes around trauma-adjacent cues rather than general triggers
The client meets PTSD criteria on the PCL-5 or has substantial sub-threshold trauma-stress features
ERP has made real compulsion-level gains but has plateaued on background distress
No single sign is sufficient; two or three together shift the formulation.
When pure ERP is the better path
By contrast, when the obsessional content does not track to a specific memory, when the client reports no meaningful trauma history, and when ERP is producing steady week-over-week gains, adding EMDR is usually the wrong move. It extends treatment length, divides clinical attention, and can inadvertently introduce new content into the system.
When EMDR happens before, during, or after ERP
Sequencing varies. For clients whose trauma symptoms are so elevated that ERP sessions are being destabilized by them, stabilization-phase EMDR — or adjacent trauma-focused work in our trauma services — can come first. For clients whose ERP is producing uneven gains, EMDR can be interleaved on specific target memories. For clients whose ERP has completed and produced a plateau on background distress, EMDR can be the next phase rather than the first phase.
Four questions to ask a clinician before adding EMDR
If you are being offered combined EMDR + ERP, or evaluating whether to add EMDR to an ongoing OCD plan, these are concrete questions to raise:
What in my presentation is suggesting that ERP alone will not be sufficient, and what specifically would EMDR be targeting?
Are you trained in both modalities, or would I be working with two clinicians, and how is coordination handled?
If EMDR destabilizes me, what is the plan — do we pause ERP, change the pacing, or shift back to stabilization work?
How will we measure whether the addition of EMDR is actually helping, and at what point would we reconsider?
Those four questions will tell you a lot about the clinician's thinking and about the quality of the treatment plan.
OCD subtypes where EMDR-as-adjunct is most commonly considered
Contamination OCD with medical or abuse history
Contamination OCD is one of the best-studied subtypes and typically responds well to ERP alone. The subset where adding EMDR is reasonable is narrower: contamination fears that trace to medical trauma (poorly handled procedures in childhood, significant medical events), caregiver contamination dynamics, or experiences of physical or sexual abuse where the contamination content carries clear thematic echoes of the trauma.
Harm OCD with prior traumatic exposure
Harm OCD — intrusive thoughts about hurting oneself or others — similarly responds to high-quality ERP in most cases. Adjunct EMDR is most often considered when the harm content tracks to a specific prior event: witnessing violence, a significant relational trauma involving loss of control, or an incident where the client was the object of someone else's harm.
Relationship OCD (ROCD)
Relationship OCD is complex because much of the relevant clinical material — attachment history, prior relational ruptures, formative romantic experiences — is memory-network adjacent by default. That does not mean every ROCD client needs EMDR; most do not. It means that when ROCD does not respond well to ERP, the first place to look is usually the relational history, and EMDR is one of the tools in that exploration.
Key takeaway: 🎯 The common thread across subtypes where EMDR is reasonably added is that the obsessional content is anchored to a specific, identifiable memory — not a general life theme.
Using the Y-BOCS to benchmark severity and track progress
Before any decision about whether to add EMDR to an OCD treatment plan, we want a shared, objective read on where OCD severity sits. The OCD symptom screener is the standard instrument for this. It produces a 0-to-40 severity score — subclinical, mild, moderate, severe, extreme — based on time spent, interference, distress, resistance, and control across both obsessions and compulsions [11]. Running it at baseline, at regular intervals during ERP, and before any treatment plan change gives clinician and client a shared dashboard.
Where the Y-BOCS is most useful in the EMDR-adjunct decision is in the trajectory: not the absolute score but the slope. A client whose Y-BOCS has steadily declined over twelve weeks of ERP likely does not need EMDR added. A client whose Y-BOCS has plateaued in the moderate range despite competent ERP, and who can identify specific memory-linked content, is the kind of client for whom the EMDR conversation is worth having.
Key takeaway: 📈 Y-BOCS trajectory — not a single score — is the most useful signal for whether ERP alone is sufficient. Plateau plus identifiable trauma-linked content is the combination that makes EMDR worth discussing.

Mechanism differentiation: where ERP and EMDR actually differ
When both modalities are on the table, it helps to say plainly what each is doing. ERP works on the behavior-reinforcement loop: the client learns, through repeated exposure without compulsion, that the feared outcome does not follow and that their anxiety subsides on its own. EMDR works on memory consolidation: the client, with bilateral stimulation, brings a specific distressing memory back into an active state and the network around it appears to re-consolidate with lower affective charge [12]. In practice this means ERP is the right choice when the cycle itself is the problem, and EMDR is the right adjunct when the memory network underneath the cycle is driving some of the charge.
These mechanisms can interact well — EMDR can lower the baseline reactivity that makes exposures feel impossibly aversive, and completed exposures can lower the charge on the surface content that EMDR is working underneath. When they are working together well, each buys ground the other could not.
Frequently asked questions
Can I do EMDR if I've never tried ERP?
Usually we would recommend starting with ERP, since it has the strongest evidence for OCD and a clearer mechanism in the disorder. The exception is when trauma-stress features are so prominent that ERP would be destabilized by them, in which case stabilization-phase trauma work can come first.
Will EMDR trigger OCD themes I'd rather leave alone?
EMDR can temporarily activate distress between sessions, and for OCD clients that activation can include increased intrusive content. A competent EMDR therapist working with OCD clients plans for this, paces sessions carefully, and coordinates with the ERP clinician if there are two. It is a known consideration, not a reason to avoid the modality entirely.
Does EMDR cure OCD?
No single treatment "cures" OCD. The realistic goal for most clients is substantial, durable reduction in symptom burden — measured on the Y-BOCS and on functional metrics. EMDR contributes to that goal for the subset of clients we have been describing; it is not positioned as a cure by any clinical body.
How do I find a clinician trained in both ERP and EMDR?
Ask directly. Any clinician comfortable treating OCD should be able to tell you about their ERP training (supervision hours, IOCDF affiliations) and their EMDR training (EMDRIA-consistent basic training, consultation hours, any OCD-specific workshops). You can also reach out to the ScienceWorks team to discuss care coordination.
Next step: talking to a clinician about whether to add EMDR to OCD treatment
If you are in active ERP and curious about whether EMDR belongs in your plan, the right conversation is with the clinician who is already delivering your OCD care. If you are not yet in treatment and are trying to figure out where to start, we suggest starting with an OCD-focused evaluation; EMDR decisions can follow once there is a shared read on the clinical picture. Our practice delivers both ERP-based OCD care and EMDR for trauma-linked OCD presentations, and intake conversations can cover the full picture rather than forcing a premature choice between the two.
Frequently Asked Questions
Is ERP or EMDR better for OCD?
ERP (Exposure and Response Prevention) is the first-line psychological treatment for OCD per the IOCDF, APA, and NICE guidelines, and should not be skipped in favor of EMDR. EMDR earns a place in the treatment plan when the obsessional content is anchored to a specific identifiable memory or when ERP has plateaued despite competent delivery. The two approaches target different mechanisms — the cycle (ERP) versus the memory network (EMDR) — and work best in sequence or combination, not as substitutes. [IOCDF; NICE CG31]
Is EMDR an appropriate treatment for OCD?
EMDR is appropriate for OCD when a trauma-link is identifiable: when OCD onset coincided with a traumatic event, when obsessional content tracks thematically to a specific memory, or when ERP has produced compulsion-level gains but background distress around trauma-adjacent cues remains high. EMDR is not positioned as a first-line OCD monotherapy by any major clinical guideline. The decision to add it is usually made after enough ERP has been done to see what content the ERP is not reaching. [Marsden 2018; Scelles 2021]
Can trauma cause OCD or make it worse?
There is a well-documented relationship between early-life adversity, traumatic experience, and OCD onset and severity. A meaningful proportion of people with OCD also meet criteria for PTSD — co-occurrence estimates range from roughly 19 to 41 percent across adult samples. The relationship appears bidirectional: trauma can precipitate or intensify OCD, and OCD can magnify the distress of traumatic memory. Not every OCD case involves trauma, but when it does, the formulation often calls for trauma-informed treatment alongside ERP. [Brander 2016; Huppert 2005]
About the Author
Dr. Kiesa Kelly is a licensed clinical psychologist and the founder of ScienceWorks Behavioral Healthcare. Her clinical training includes coursework and supervised practice at the University of Chicago, Vanderbilt University, and the University of Wisconsin, with more than 20 years of experience in psychological assessment and evidence-based treatment. Her work emphasizes the interface of anxiety-spectrum conditions (OCD, generalized anxiety, PTSD) with neurodevelopmental and mood presentations, with a particular focus on differential diagnosis and treatment planning for complex adult cases.
Dr. Kelly oversees clinical quality across ScienceWorks, including the practice's OCD and trauma programs. She maintains ongoing consultation and continuing education in ERP, EMDR, and integrated trauma-informed OCD care, and every article on the ScienceWorks blog is reviewed by a licensed clinician for clinical accuracy before publication.
References
1. International OCD Foundation. Clinical Information and Resources on OCD Treatment. https://iocdf.org/expert-opinions/expert-opinion-adult-ocd-treatment/
2. Koran LM, et al. Practice guideline for the treatment of patients with obsessive-compulsive disorder. American Journal of Psychiatry. 2007 (with subsequent APA updates). https://doi.org/10.1176/appi.ajp.164.7.952
3. National Institute for Health and Care Excellence. Obsessive-compulsive disorder and body dysmorphic disorder (CG31). 2005 (current guidance). https://www.nice.org.uk/guidance/cg31
4. Marsden Z, et al. A randomized controlled trial comparing EMDR and CBT for obsessive-compulsive disorder. Clinical Psychology & Psychotherapy. 2018. https://doi.org/10.1002/cpp.2120
5. Böhm K, Voderholzer U. Use of EMDR in the treatment of obsessive-compulsive disorders: a case series. Verhaltenstherapie. 2010. https://doi.org/10.1159/000319439
6. Scelles C, Bulnes LC. EMDR as treatment option for conditions other than PTSD: a systematic review. Frontiers in Psychology. 2021. https://doi.org/10.3389/fpsyg.2021.644369
7. Craske MG, et al. Optimizing inhibitory learning during exposure therapy. Behaviour Research and Therapy. 2014. https://doi.org/10.1016/j.brat.2014.04.006
8. Brander G, et al. Systematic review of environmental risk factors for obsessive-compulsive disorder. Neuroscience & Biobehavioral Reviews. 2016. https://doi.org/10.1016/j.neubiorev.2016.04.011
9. Huppert JD, et al. The relationship between obsessive-compulsive and posttraumatic stress symptoms in clinical and non-clinical samples. Journal of Anxiety Disorders. 2005 (plus meta-analytic updates). https://doi.org/10.1016/j.janxdis.2004.02.003
10. Nazari H, et al. Comparison of eye movement desensitization and reprocessing with citalopram in treatment of obsessive-compulsive disorder. International Journal of Psychiatry in Clinical Practice. 2011. https://doi.org/10.3109/13651501.2011.607143
11. Goodman WK, et al. The Yale-Brown Obsessive Compulsive Scale (Y-BOCS): development, use, and reliability. Archives of General Psychiatry. 1989 (plus validation literature). https://doi.org/10.1001/archpsyc.1989.01810110048007
12. Landin-Romero R, et al. How does eye movement desensitization and reprocessing therapy work? A systematic review on suggested mechanisms of action. Frontiers in Psychology. 2018. https://doi.org/10.3389/fpsyg.2018.01395
Disclaimer
This article is for informational purposes only and is not a substitute for individualized medical, psychological, or psychiatric advice, diagnosis, or treatment. Reading this article does not create a clinician-client relationship. If you are experiencing a mental health emergency, call or text 988 (the Suicide and Crisis Lifeline in the United States) or go to your nearest emergency department.