
EMDR vs CPT: How Two Evidence-Based Trauma Therapies Compare
- Kiesa Kelly

- Apr 22
- 14 min read
Last reviewed: 06/03/2026
Reviewed by: Dr. Kiesa Kelly

If you've been researching trauma treatment, two names keep coming up: EMDR and CPT. Both are strongly recommended for post-traumatic stress disorder (PTSD). Both have decades of research behind them. And both work — studies have found that roughly 60 to 70 percent of people who complete a full course of either therapy no longer meet criteria for PTSD afterward [1][2]. The real question most readers bring to "emdr vs cpt" isn't which one works. It's which one is a better fit for them.
This guide is written for people trying to make that decision without a clinical degree. We'll compare mechanisms, session structure, guideline ratings, and the client profiles each approach tends to suit best. If you already know you want to pursue Eye Movement Desensitization and Reprocessing, you can start with our overview of EMDR and bilateral stimulation. If you're still early in the decision, keep reading.
In this article, you'll learn:
How EMDR and Cognitive Processing Therapy (CPT) actually differ in mechanism and protocol
What the APA and VA/DoD PTSD guidelines say about each
Which client profiles tend to fit EMDR better, and which tend to fit CPT
Why the "CPT" you type into Google might be the billing code, not the therapy
How EMDR and CPT compare to related options like ACT, ERP, and prolonged exposure
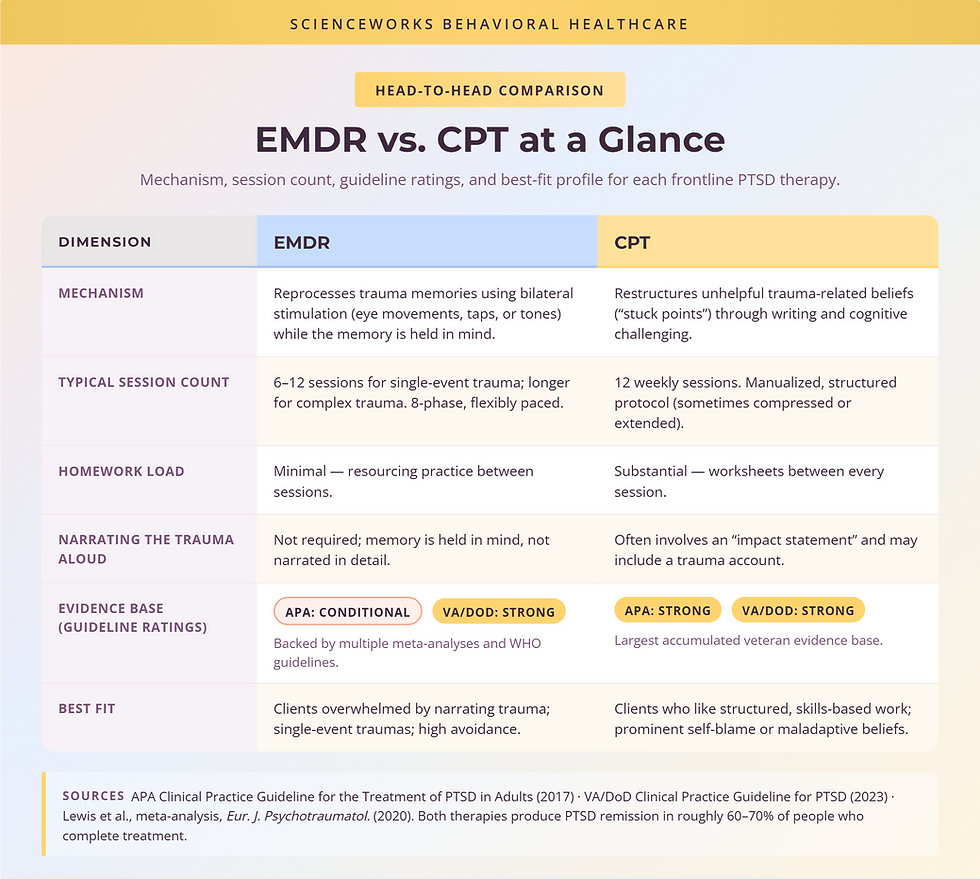
EMDR vs. CPT at a glance
Full name
EMDR: Eye Movement Desensitization and Reprocessing. CPT: Cognitive Processing Therapy.
Core mechanism
EMDR: Reprocesses trauma memories using bilateral stimulation (eye movements, taps, or tones) while holding the memory in mind [3]. CPT: Restructures unhelpful trauma-related beliefs ("stuck points") through writing and cognitive challenging [4].
Structure
EMDR: 8-phase protocol, flexibly paced. CPT: 12-session structured protocol.
Typical length
EMDR: 6–12 sessions for single-event trauma; longer for complex trauma [3]. CPT: 12 weekly sessions (sometimes compressed or extended) [4].
Homework load
EMDR: Minimal. CPT: Substantial — worksheets between every session.
Talking about the trauma in detail
EMDR: Not required; the memory is held in mind rather than narrated aloud. CPT: Often involves writing an "impact statement" and, in some versions, a trauma account.
APA PTSD guideline rating
EMDR: Conditionally recommended [5]. CPT: Strongly recommended [5].
VA/DoD PTSD guideline rating
EMDR: Strongly recommended [6]. CPT: Strongly recommended [6].
Typical best fit
EMDR: Clients who feel overwhelmed narrating trauma; single-event traumas; high avoidance. CPT: Clients who respond well to structured, skills-based work; prominent self-blame or maladaptive beliefs.
Both therapies are considered frontline treatments. The differences below determine fit, not effectiveness.
Key takeaway: 🧭 Head-to-head trials have not shown a reliable winner between EMDR and CPT. When both are delivered by well-trained clinicians, effect sizes are comparable [2][7]. Fit matters more than ranking.
What CPT is — quick explainer
Cognitive Processing Therapy was developed in the late 1980s by Dr. Patricia Resick, originally for survivors of sexual assault, and has since been adapted for veterans, refugees, and survivors of many trauma types [4]. It's one of two trauma-focused cognitive behavioral therapies that carry the American Psychological Association's "strongly recommended" rating for PTSD [5].
The 12-session structured protocol
CPT is manualized. That means every session has a purpose, and the overall arc is predictable: psychoeducation about PTSD in the first couple of sessions, an "impact statement" about how the trauma changed your beliefs about yourself and the world, worksheets that help you identify distorted thoughts, and then several sessions of progressively more sophisticated cognitive challenging around themes like safety, trust, power/control, esteem, and intimacy [4][8].
The structured pacing is a feature, not a bug. Many clients find that knowing what comes next reduces the dread of each session. You'll know in week 3 what week 9 will look like. For people who find ambiguity intolerable, this is a meaningful advantage.
Stuck points and cognitive restructuring
The central idea in CPT is the "stuck point" — a belief the trauma installed or reinforced that now gets in the way of healing. Common stuck points include "It was my fault," "I can't trust anyone," "I should have known," or "The world is completely dangerous." The therapy teaches you to examine these beliefs the way a scientist examines a hypothesis: What's the evidence? What's the counter-evidence? Is this belief serving you now, or costing you?
Key takeaway: 📋 CPT is structured, homework-heavy, and focused on changing trauma-related beliefs. It does not require you to repeatedly narrate the trauma in detail — a distinction that matters for many clients.

What EMDR is — quick explainer
EMDR was developed by Francine Shapiro in 1987 after she noticed that her own distressing thoughts softened when she moved her eyes back and forth. Forty years of research later, it's recommended by the World Health Organization, the VA/DoD, and (conditionally) the APA for PTSD [5][6][9].
The 8-phase protocol
EMDR moves through eight phases: history-taking, preparation and resourcing, assessment of target memories, desensitization (the part with bilateral stimulation), installation of adaptive beliefs, body scan, closure, and re-evaluation [3]. For a closer look at what bilateral stimulation actually feels like and how the eight phases unfold in practice, see our detailed explainer on the EMDR protocol and bilateral stimulation.
Unlike CPT, EMDR is not strictly time-limited. Single-event adult trauma often resolves in 6 to 12 sessions. Complex, long-standing, or developmental trauma typically takes longer, and good clinicians will not rush the preparation phase [3][10].
Bilateral stimulation and memory reprocessing
During desensitization, you hold the trauma memory in mind — image, emotion, body sensation, and the negative belief attached to it — while the clinician guides your eyes back and forth (or delivers alternating taps or tones). The current leading explanation is that bilateral stimulation taxes working memory in a way that reduces the vividness and emotional charge of the memory each time it's recalled [11]. You don't have to narrate the trauma in detail; you just have to hold it in mind long enough for the brain to reprocess it.
For many clients, this is the single most important difference between the two therapies. EMDR asks less of your capacity to talk about what happened.
Key takeaway: 🌀 EMDR reprocesses trauma memories through bilateral stimulation while you hold the memory in mind. It is less narrative-heavy than most other trauma therapies.
Where the evidence lines up — and where it differs
APA PTSD guideline ratings for each
The 2017 APA Clinical Practice Guideline for the Treatment of PTSD in Adults places CPT in the "strongly recommended" tier alongside prolonged exposure and trauma-focused CBT. EMDR is in the "conditionally recommended" tier — a step below, but still recommended [5]. The conditional rating reflects smaller total evidence base at the time, not a negative finding; multiple meta-analyses since have reinforced EMDR's effectiveness [2][9].
VA/DoD guideline recommendations
The VA/DoD Clinical Practice Guideline for PTSD (most recently updated in 2023) rates both CPT and EMDR as strongly recommended, along with prolonged exposure [6]. For veterans specifically, CPT has the largest accumulated evidence base, but EMDR is routinely offered and, for some veterans, is the preferred first-line choice — particularly those whose avoidance makes extended verbal processing of combat memories difficult [6][12].
Symptom-reduction speed vs. long-term maintenance
Head-to-head trials tend to show similar endpoint outcomes between EMDR and CPT, with both producing large reductions in PTSD symptoms and maintained gains at 6- and 12-month follow-up [2][7]. Some studies suggest EMDR produces faster early symptom reduction for single-event trauma, while CPT produces particularly durable changes in trauma-related cognitions [7][13]. Neither difference is large enough to pick a winner across the board.
Key takeaway: 🧪 APA rates CPT "strongly recommended" and EMDR "conditionally recommended"; VA/DoD strongly recommends both. At the individual level, both work for roughly 6 to 7 out of 10 people who complete a course [1][2].
When EMDR is usually the better fit
Avoidant or overwhelmed clients
Avoidance is a core PTSD symptom, not a personal failing — and for some people, the prospect of writing out detailed trauma accounts or sitting with extended verbal processing is genuinely intolerable. If you've tried therapy before and bailed because the "talking about it" part felt worse than the symptoms, EMDR is often a more workable entry point. You hold the memory in mind, but you are not asked to narrate it in detail.
Worked example. You were in a serious car accident two years ago. You can describe the basics — date, intersection, the other driver — but every time a therapist asks you to go deeper, your chest tightens and you feel like you're going to pass out. You've stopped booking therapy appointments because the night before each one, you can't sleep. In EMDR, your clinician would spend the first phases helping you build internal resources (calm place, container imagery, grounding skills) before any target memory is approached. When desensitization begins, you hold the memory in mind silently; you don't have to walk your therapist through it. Many clients who couldn't get through exposure-based protocols find they can get through this one.
Single-event trauma
The EMDR evidence base is particularly strong for discrete, identifiable traumas: accidents, assaults, medical events, natural disasters [3][9]. For adults with otherwise stable lives who experienced a single event, EMDR often resolves symptoms in fewer sessions than longer-protocol therapies.
Worked example. You were mugged at knifepoint six months ago and haven't felt safe walking in your neighborhood since. You startle at footsteps behind you, avoid the block where it happened, and have replayed the moment the knife appeared hundreds of times. You're functioning at work but not sleeping well. In EMDR, that specific memory would become a target. Many clients in this situation see meaningful symptom reduction within 6 to 10 sessions [3].
Clients who don't want to narrate trauma in detail
This is the same point as the avoidance example, but it's worth stating separately because it applies to people who are not avoidant in the clinical sense — they're just private, or the trauma involves content (sexual assault, loss of a child, combat) they do not want to speak aloud repeatedly. EMDR respects that. The memory lives in your head; your therapist does not need the transcript.
The distinguishing pattern: EMDR tends to be the better fit when the cost that's blocking treatment is the cost of telling the story — emotional, verbal, or narrative load. If talking about the trauma is what stopped you from getting help, start here.
When CPT is usually the better fit
Clients who want structured, skills-based tools
If you're the kind of person who likes worksheets, homework, and knowing the syllabus, CPT's 12-week structure is a feature. You'll build a concrete skill — examining and challenging thoughts — that you keep after therapy ends. Many clients describe CPT as feeling more like "doing something" than "processing something," and for certain temperaments that's the match.
Worked example. You're a first responder who has been through multiple critical incidents over a 15-year career. You don't think you have one "target memory" — you have a generalized belief that the world is dangerous and people are unreliable, and it's costing you in your marriage. In CPT, you'd work through the five theme sessions (safety, trust, power/control, esteem, intimacy) and learn to recognize when these beliefs are firing in daily life. You'd leave therapy with a durable cognitive toolkit.
Prominent self-blame or maladaptive trauma beliefs
When trauma produces pervasive self-blame ("I should have fought back," "I should have known") or global negative beliefs about the world ("No one can be trusted"), directly restructuring those beliefs is often the most efficient path. CPT was built for exactly this work, and outcome studies show particularly strong effects on trauma-related guilt and self-blame [4][13].
Worked example. You were in an abusive relationship for years and have been out of it for 18 months. The flashbacks have faded, but what remains is a loud internal voice telling you that you chose it, you stayed too long, and something is fundamentally wrong with you. A friend who survived similar circumstances did CPT and said the worksheets "were the only thing that ever got her out of her own head." You're intellectually oriented, comfortable with writing, and curious about why you believe what you believe. CPT tends to suit this profile well.
The distinguishing pattern: CPT tends to be the better fit when the cost that remains after the trauma is belief-based — self-blame, distorted meaning, broken assumptions about safety or trust. If the intrusive memories have faded but the beliefs have not, CPT's cognitive engine is built for that work.
Quick note on "CPT" billing codes vs. CPT therapy
A note for anyone who arrived here via a "CPT code" search: the acronym does double duty. In this article, CPT means Cognitive Processing Therapy — the trauma therapy described above. In medical billing, CPT stands for Current Procedural Terminology, the standardized codes (maintained by the American Medical Association) that providers use to bill insurance for services [14].
EMDR and Cognitive Processing Therapy are both typically billed under standard psychotherapy CPT codes such as 90832, 90834, or 90837 (for 30-, 45-, or 60-minute individual therapy, respectively). There is no dedicated "EMDR CPT code" or "CPT therapy CPT code" — the billing code reflects the length and type of session, not the specific therapeutic modality [14]. If you're checking insurance coverage, ask whether your plan covers outpatient psychotherapy under those codes; it almost always does.
Key takeaway: 🧾 "CPT code" in insurance contexts means the billing code. "CPT therapy" means Cognitive Processing Therapy. EMDR and CPT therapy are both billed under standard psychotherapy codes.
Frequently asked questions
Can I combine EMDR and CPT?
Yes, and many clinicians do. Some EMDR therapists integrate cognitive restructuring during the installation phase; some CPT therapists use EMDR-style resourcing in early sessions. Pure-protocol purists exist in both camps, but most experienced trauma clinicians draw from both toolkits as the client's needs change [15]. It's reasonable to ask a prospective therapist how they think about sequencing or integrating the two.
Which has better long-term outcomes?
Follow-up studies at 6, 12, and (in some cases) 24 months show that both therapies produce durable gains — the majority of people who responded at the end of treatment are still responding a year later [2][7][13]. Where small differences have emerged, they tend to be on specific outcome measures (e.g., CPT's edge on trauma-related cognitions) rather than on overall PTSD symptom severity.
What about ACT, ERP, or prolonged exposure?
Prolonged Exposure (PE) is the third strongly recommended trauma therapy in both APA and VA/DoD guidelines alongside CPT, and is comparable in effectiveness to EMDR and CPT in head-to-head trials [5][6]. Acceptance and Commitment Therapy (ACT) is sometimes used adjunctively for trauma but does not yet have the same guideline status; the evidence base is promising but smaller [16]. Exposure and Response Prevention (ERP) is the frontline treatment for OCD, not PTSD — if intrusive thoughts have compulsive features and the picture looks more like OCD than PTSD, our OCD services page is a better starting place.
Will insurance cover one but not the other?
Because both EMDR and CPT are billed under standard psychotherapy CPT codes, commercial insurance typically covers them the same way — subject to the plan's mental health benefits and the provider being in-network or eligible for out-of-network reimbursement [14]. Some plans may not reimburse for EMDR if the provider isn't certified; we recommend asking the provider directly what coverage looks like for your specific plan.
What the First Few Sessions Look Like in Each
Both therapies start with preparation, not the hardest material — a detail that surprises people who expect to "dive into the trauma" on day one.
In CPT, the opening sessions are largely psychoeducation: your therapist explains how PTSD keeps trauma "stuck" and introduces the idea of stuck points. Early on you'll usually write a short impact statement about why you think the trauma happened and how it changed your view of yourself, others, and the world. From there, sessions follow a predictable weekly arc with worksheets between them. You'll generally know in week 3 roughly what week 9 will involve — many people find that predictability lowers the dread.
In EMDR, the first sessions are history-taking and preparation and resourcing — building grounding and calming skills and a sense of safety before any memory is reprocessed. You won't be asked to narrate the trauma in detail; when reprocessing begins, you hold the memory in mind while the clinician guides sets of bilateral stimulation, pausing frequently to check in. The pace is flexible and reprocessing only starts once preparation is solid.
The shared theme: in both, the early work is about building footing. If reading these two descriptions, one already sounds more tolerable than the other, that reaction is useful information to bring to a first conversation with a therapist.
Next step: deciding which trauma therapy is right for you
Here's a working heuristic, not a substitute for clinical judgment:
If talking about the trauma in detail is the barrier that's stopped you from getting help, or if your trauma is a discrete event you can clearly identify, EMDR is often the better first move. Start with our EMDR and bilateral stimulation overview to learn what the eight phases actually look like in session.
If what remains after the trauma is a pervasive belief — about yourself, other people, or the world — and you want a structured, skills-based approach you can take with you, CPT is often the better first move. You can read more about our broader trauma services and treatment options.
If your symptoms are severe, new, or you're unsure whether PTSD is the right frame at all, start by completing the PCL-5 self-screening and bringing the result to a clinician. The PCL-5 is the most widely validated PTSD self-report measure [17] and gives a provider a concrete starting point.
If you have co-occurring concerns — chronic depression, active substance use, dissociation, complex developmental trauma — the choice of therapy should follow a full evaluation, not a blog post. Our specialized therapy services page describes how we sequence treatment when the picture is layered.
Questions worth asking any trauma therapist in a first conversation:
Are you formally trained in EMDR (EMDRIA-approved) and/or CPT (Resick-model)?
How do you decide between protocols when a new client could fit either?
What does your preparation or resourcing phase look like before we approach any target memories?
How do you sequence treatment when there are co-occurring conditions like depression, substance use, or dissociation?
If you'd like help thinking through which approach fits your situation — or you already know you want to begin with EMDR — you can reach out to our team and we'll help you take the next step.
About the Author
Dr. Kiesa Kelly is a licensed clinical psychologist and the founder of ScienceWorks Behavioral Healthcare. Her clinical work focuses on psychological assessment and evidence-based treatment of trauma, anxiety, OCD, ADHD, and autism across adolescents and adults. She completed her doctoral training in clinical psychology and has more than 20 years of experience delivering and supervising evidence-based psychotherapies, including trauma-focused cognitive behavioral therapy and EMDR-informed care. Her clinical training includes work at the University of Chicago, Vanderbilt University, and the University of Wisconsin.
Dr. Kelly reviews every clinical article published by ScienceWorks for accuracy before it goes live. She is a strong advocate for matching clients to the evidence-based therapy most likely to fit their profile — not the therapy a clinician happens to be most comfortable delivering.
References
1. Cusack K, Jonas DE, Forneris CA, et al. Psychological treatments for adults with posttraumatic stress disorder: A systematic review and meta-analysis. Clinical Psychology Review. 2016;43:128–141. https://pubmed.ncbi.nlm.nih.gov/26574151/
2. Lewis C, Roberts NP, Andrew M, Starling E, Bisson JI. Psychological therapies for post-traumatic stress disorder in adults: systematic review and meta-analysis. European Journal of Psychotraumatology. 2020;11(1):1729633. https://doi.org/10.1080/20008198.2020.1729633
3. Shapiro F. The role of Eye Movement Desensitization and Reprocessing (EMDR) therapy in medicine: addressing the psychological and physical symptoms stemming from adverse life experiences. The Permanente Journal. 2014;18(1):71–77. https://doi.org/10.7812/TPP/13-098
4. Resick PA, Monson CM, Chard KM. Cognitive Processing Therapy for PTSD: A Comprehensive Manual. New York: Guilford Press; 2017. https://www.guilford.com/books/Cognitive-Processing-Therapy-for-PTSD/Resick-Monson-Chard/9781462533671
5. American Psychological Association. Clinical Practice Guideline for the Treatment of Posttraumatic Stress Disorder (PTSD) in Adults. 2017. https://www.apa.org/ptsd-guideline/ptsd.pdf
6. U.S. Department of Veterans Affairs and Department of Defense. VA/DoD Clinical Practice Guideline for the Management of Posttraumatic Stress Disorder and Acute Stress Disorder. 2023. https://www.healthquality.va.gov/guidelines/MH/ptsd/
7. Rosner R, Rimane E, Frick U, et al. Effect of Developmentally Adapted Cognitive Processing Therapy for Youth With Symptoms of Posttraumatic Stress Disorder After Childhood Sexual and Physical Abuse: A Randomized Clinical Trial. JAMA Psychiatry. 2019;76(5):484–491. https://doi.org/10.1001/jamapsychiatry.2018.4349
8. Asmundson GJG, Thorisdottir AS, Roden-Foreman JW, et al. A meta-analytic review of cognitive processing therapy for adults with posttraumatic stress disorder. Cognitive Behaviour Therapy. 2019;48(1):1–14. https://doi.org/10.1080/16506073.2018.1522371
9. World Health Organization. Guidelines for the Management of Conditions Specifically Related to Stress. 2013. https://www.who.int/publications/i/item/9789241505406
10. Korn DL. EMDR and the treatment of complex PTSD: A review. Journal of EMDR Practice and Research. 2009;3(4):264–278. https://doi.org/10.1891/1933-3196.3.4.264
11. van den Hout MA, Engelhard IM. How does EMDR work? Journal of Experimental Psychopathology. 2012;3(5):724–738. https://doi.org/10.5127/jep.028212
12. Haagen JFG, Smid GE, Knipscheer JW, Kleber RJ. The efficacy of recommended treatments for veterans with PTSD: A meta-regression analysis. Clinical Psychology Review. 2015;40:184–194. https://doi.org/10.1016/j.cpr.2015.06.008
13. Resick PA, Wachen JS, Dondanville KA, et al. Effect of Group vs Individual Cognitive Processing Therapy in Active-Duty Military Seeking Treatment for Posttraumatic Stress Disorder: A Randomized Clinical Trial. JAMA Psychiatry. 2017;74(1):28–36. https://doi.org/10.1001/jamapsychiatry.2016.2729
14. American Medical Association. CPT (Current Procedural Terminology) Overview. https://www.ama-assn.org/practice-management/cpt
15. Maxfield L, Hyer L. The relationship between efficacy and methodology in studies investigating EMDR treatment of PTSD. Journal of Clinical Psychology. 2002;58(1):23–41. https://doi.org/10.1002/jclp.1127
16. Lang AJ, Schnurr PP, Jain S, et al. Randomized controlled trial of Acceptance and Commitment Therapy for distress and impairment in OEF/OIF/OND veterans. Psychological Trauma. 2017;9(S1):74–84. https://doi.org/10.1037/tra0000127
17. Blevins CA, Weathers FW, Davis MT, Witte TK, Domino JL. The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and initial psychometric evaluation. Journal of Traumatic Stress. 2015;28(6):489–498. https://doi.org/10.1002/jts.22059
Disclaimer
This article is for informational and educational purposes only and is not a substitute for individualized clinical advice, diagnosis, or treatment. Reading this content does not establish a clinician–patient relationship. If you are experiencing a mental health crisis or thoughts of harming yourself, please contact the 988 Suicide and Crisis Lifeline or go to your nearest emergency department. Treatment decisions should be made in collaboration with a licensed clinician who can evaluate your individual history and circumstances.