
High-Functioning Depression: PDD vs. MDD | ScienceWorks
- Kiesa Kelly

- 4 days ago
- 11 min read
Updated: 3 days ago
Last reviewed: 07/05/2026
Reviewed by: Dr. Kiesa Kelly

You get up, go to work, answer the emails, keep the household running, and to everyone around you, you seem fine. Underneath, though, there is a low, steady weight that rarely lifts — a flatness, a fatigue, a quiet sense that you are running on fumes and have been for a long time. Many people call this "high-functioning depression." It is a real experience with a confusing name, because the term is not actually a medical diagnosis. Understanding what it usually points to — and how that differs from major depression — can help you decide whether it is time to get a closer look.
In this article, you'll learn:
What "high-functioning depression" really means, and why it is not a formal diagnosis
How persistent depressive disorder (PDD) differs from major depressive disorder (MDD)
The everyday signs that a low mood has become something more than stress
Common misconceptions that keep people from seeking help
How depression is assessed, and what treatment actually looks like
A simple way to decide whether an evaluation makes sense for you
The central tension is this: the very thing that makes this kind of depression easy to overlook — the fact that you are still functioning — is also what lets it quietly persist for years. Naming it accurately is the first step toward doing something about it.
What "high-functioning depression" really means
"High-functioning depression" is a plain-language term, not a clinical one. You will not find it in the DSM-5, the manual clinicians use to make diagnoses [1]. It describes a recognizable pattern — ongoing depressive symptoms paired with a preserved ability to work, parent, and meet obligations — but it is a description, not a disorder in its own right. The most useful thing to understand is what the label usually points to underneath.
In most cases, the diagnosis that best fits this pattern is persistent depressive disorder (PDD), once known as dysthymia [1]. If you are trying to make sense of your own symptoms, a validated screener like the PHQ-9 depression screener can give you a structured snapshot of how heavy things have been lately, which is a helpful starting point before a conversation with a clinician. PDD is a chronic, lower-grade form of depression: the symptoms are often milder than a full major depressive episode, but they last far longer — two years or more, with few genuine breaks [1][10].
It is worth being precise here, because the research is still developing. Some recent clinical writers argue that "high-functioning depression" is not perfectly synonymous with PDD — that it captures a group of people who stay so busy and outwardly successful that they do not even report feeling depressed, which is subtly different from the classic dysthymia picture [3][4]. In other words, the label is a bridge to a clinical conversation, not a substitute for one. The experiential side of this — what it feels like to carry it — is covered in our companion piece on what high-functioning depression feels like day to day; this article focuses on the diagnostic side.
Key takeaway: 🏷️ "High-functioning depression" is a nickname for a real experience, but the condition a clinician actually diagnoses and treats is usually persistent depressive disorder.
PDD vs. MDD: the distinction that matters
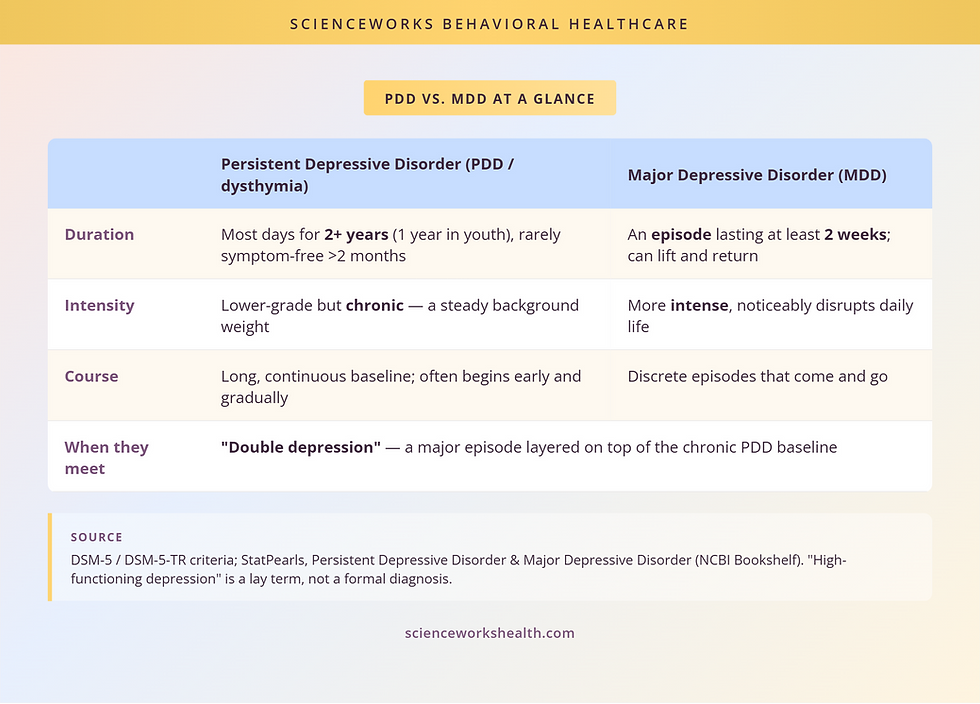
The clearest way to separate persistent depressive disorder from major depressive disorder is to think about duration and intensity rather than a simple "mild versus serious" scale.
Major depressive disorder tends to arrive in episodes. To meet criteria, symptoms have to be present for at least two weeks, and they are usually intense enough to visibly disrupt daily life — a marked drop in mood or loss of interest, along with changes in sleep, appetite, energy, concentration, and self-worth [2]. Episodes can lift and return.
Persistent depressive disorder works differently. The defining feature is chronicity: a depressed mood most of the day, more days than not, for at least two years in adults (one year in children and teens), without going symptom-free for more than two months at a stretch [1][10]. Alongside the low mood, PDD involves at least two of a familiar cluster — poor appetite or overeating, sleep trouble, low energy, low self-esteem, poor concentration, or a sense of hopelessness [1]. The intensity on any given day may be lower than a major episode, but the sheer length is what does the damage.
The two are not mutually exclusive. When someone with the chronic baseline of PDD also has a full major depressive episode layered on top, clinicians call it "double depression" [1]. This matters because it reframes the question. It is not always "Is it PDD or MDD?" — sometimes it is both, and recognizing the chronic layer changes the treatment plan. Depression is common in either form; national data show depressive symptoms affect a substantial and rising share of adults [12], and PDD in particular is easy to under-count precisely because people keep functioning.
Key takeaway: 📏 The line between PDD and MDD is mostly about time: MDD is defined by intense episodes lasting weeks, while PDD is defined by a lower-grade mood that persists for years.
Common misconceptions that keep people stuck
Because this kind of depression is quiet, several myths tend to keep people from taking it seriously.
"If it were real depression, I wouldn't be able to function." In reality, functioning and feeling well are not the same thing. Persistent depressive disorder is defined partly by the fact that people keep going — the diagnostic threshold is about the presence and duration of symptoms, not about whether you have stopped showing up [1]. Many people meet every obligation while carrying a heavy internal load, often by overworking to stay ahead of the flatness.
"High-functioning depression is mild, so it's not worth treating." Lower intensity does not mean low cost. Because PDD lasts for years, its cumulative burden on health, relationships, and quality of life can rival or exceed that of shorter major episodes, and leaving it unaddressed raises the risk of a full major depressive episode and of suicidality [3][4]. Chronic and quiet is not the same as harmless.
"This is just my personality — I've always been like this." PDD often begins early and gradually, so it can feel like a fixed trait rather than a treatable condition [1]. But a mood disorder that has been present since your teens or twenties is still a mood disorder, and the fact that it feels like "just you" is one of the reasons it goes undiagnosed for so long — sometimes over a decade.
Key takeaway: 🎭 Being able to keep going is not evidence that nothing is wrong; with persistent depression, functioning is exactly what hides the problem.
Signs it may be more than stress
Stress comes and goes with circumstances. Persistent depressive disorder tends to stay put even when circumstances improve. A few worked examples may help you recognize the pattern.
You have a good week — a vacation, a promotion, a stretch where nothing is going wrong — and you notice that the low, gray baseline barely moves. You are grateful on paper, but the flatness does not lift the way it seems to for other people. That gap between "my life is fine" and "I still feel weighed down" is one of the most telling signs, because it points to something internal and durable rather than a reaction to a hard patch.
Or: you get everything done, but it costs far more than it seems like it should. You push through the workday on willpower, come home depleted, and have nothing left for the people or activities you used to enjoy. You are not in crisis, and you would probably tell a doctor you are "fine," but you cannot remember the last time you felt genuinely rested or interested rather than just functional. If anxiety rides alongside the low mood — a common pairing — a quick look at a GAD-7 anxiety screener can help you and a clinician see the fuller picture, since anxiety and depression frequently travel together.
How it shows up day to day
Day to day, PDD often looks like a collection of small, chronic frictions rather than one dramatic collapse: chronically low energy, sleep that is either too little or too much, trouble concentrating or deciding, a persistent dim view of yourself, and a background hopelessness that you have learned to work around [1]. None of these on its own screams "depression," which is exactly why the pattern gets missed. It is the combination, and the fact that it has been running for years, that matters.
How depression is assessed
You cannot diagnose persistent depressive disorder from a checklist alone, but assessment is more structured than most people expect. It usually combines a validated symptom measure, a clinical interview, and a careful look at history and timeline.
Screeners come first. The PHQ-9 is a widely used, well-validated nine-item questionnaire that scores depressive symptom severity and tracks it over time [8]. It is genuinely useful — but it is a starting point, not a verdict. A high score signals that a closer look is warranted; it does not, by itself, tell you whether you are dealing with PDD, MDD, or both.
The part a screener cannot do is establish the timeline, and timeline is where the PDD-versus-MDD distinction lives. That is why a full psychological assessment matters: a clinician gathers how long the mood has lasted, whether there have been symptom-free stretches, and whether more intense episodes have layered on top of a chronic baseline. If you are choosing an evaluation, these are fair questions to ask a provider directly: How will you tell the difference between a persistent low-grade depression and a major depressive episode? What history will you gather about how long this has been going on? Will you screen for co-occurring anxiety or other conditions? And what will I actually walk away with — a label, or specific recommendations I can use?
Key takeaway: 🧭 A screener measures how heavy things feel now; a full evaluation establishes how long it has lasted — and duration is what distinguishes persistent depression from a major episode.
What actually helps
The encouraging part is that both persistent depressive disorder and major depression are treatable, and the general approach is well supported by clinical guidelines. The American Psychological Association's treatment guideline and the UK's NICE guideline for depression in adults both recommend evidence-based psychotherapy, medication, or a combination, matched to the person and the severity [5][6].
For chronic depression specifically, psychotherapy has a strong evidence base, and a recent meta-analysis suggests psychotherapy and combined treatment can hold up at least as well as medication alone over the longer term [7]. One approach, the Cognitive Behavioral Analysis System of Psychotherapy (CBASP), was developed specifically for persistent depression and is recommended in guidelines for that chronic pattern [11]. More broadly, therapy for depression that fits your history and goals — rather than a one-size-fits-all plan — tends to be where durable change comes from. Medication can also play an important role, and for many people the combination works better than either alone [5][7].
Key takeaway: 🌱 Both persistent and major depression are treatable; the chronic form may simply need more patience, because the patterns being unwound are long-standing.
What to be cautious of
A few honest cautions. First, chronic depression can respond more slowly than a short episode, precisely because the patterns are long-standing — patience and consistency matter. Second, "high-functioning" people often stop treatment early because they are used to pushing through and can talk themselves out of care once the sharpest edge is off. And third, the evidence base for the popular concept of "high-functioning depression" specifically is still emerging, so be wary of programs that market it as a distinct, tidy condition with a proprietary cure; the sound approach is to assess and treat the underlying depression [3][4][9].
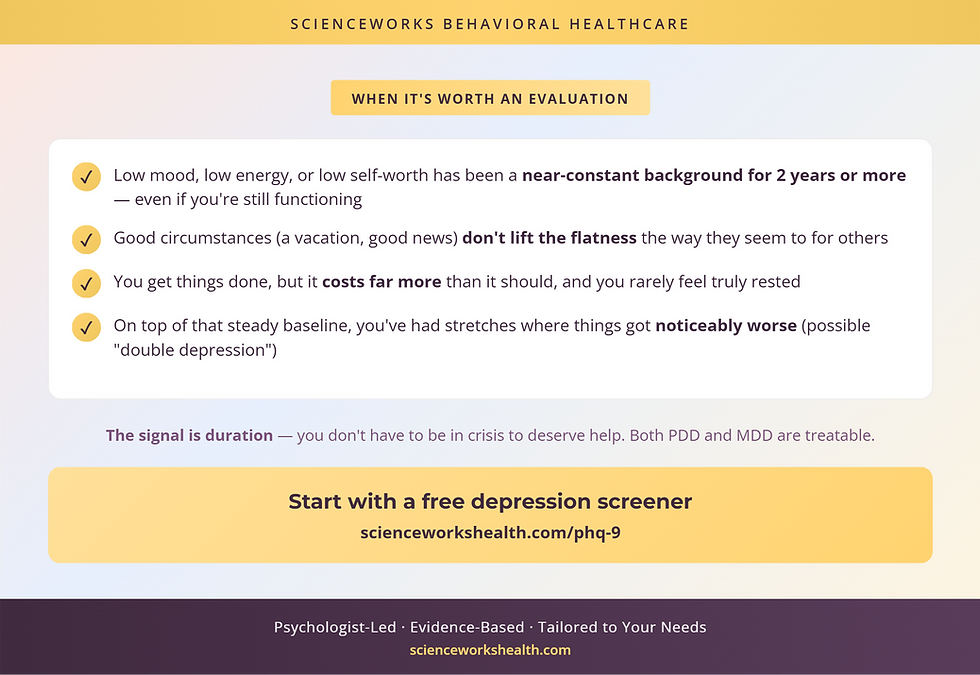
When to get evaluated
Here is a simple way to decide. If low mood, low energy, or a persistently dim view of yourself have been a near-constant background for two years or more — even though you are still functioning — that duration alone is a reason to get evaluated. You do not need to be in crisis to qualify for help. And if, on top of that steady baseline, you have had stretches where things got noticeably worse, that may be "double depression," and it is worth naming rather than waiting out.
The mistake most people in this situation make is setting the bar at "falling apart." Persistent depression rarely announces itself that way. The more accurate bar is duration: a low mood that has quietly lasted for years, and that good circumstances do not seem to fix, has already told you what you need to know.
Feeling weighed down lately? Depression is treatable, and the right support makes a difference — a clinician can help you understand what's going on and what would help you feel like yourself again.
Frequently Asked Questions
Is high-functioning depression a real diagnosis?
No. "High-functioning depression" is a popular, plain-language term, not an official diagnosis in the DSM-5. It describes people who carry ongoing depressive symptoms while still meeting daily responsibilities. The formal diagnosis it most often maps to is persistent depressive disorder (PDD), a chronic low-grade depression. The label can still be useful for talking about the experience, but a clinician diagnoses the underlying condition, not the nickname.
What is the difference between dysthymia and major depression?
The core difference is duration and intensity. Persistent depressive disorder (formerly dysthymia) is a lower-grade depression that lasts two years or more with few symptom-free breaks. Major depressive disorder tends to come in more intense episodes that last at least two weeks. PDD is often less severe day to day but far more chronic, and the two can overlap, which clinicians call "double depression."
Can you have depression and still function at work?
Yes. Holding down a job, showing up for people, and appearing "fine" does not rule out depression. In persistent depressive disorder, low mood, fatigue, and low self-worth run in the background while you keep meeting demands, often by overworking or masking. Preserved functioning is one of the main reasons this kind of depression gets missed for years, both by others and by the person living with it.
Is there a test for high-functioning depression?
There is no single test, but validated screeners like the PHQ-9 can measure depressive symptom severity and track it over time. A screener is a starting point, not a diagnosis. A full evaluation adds a clinical interview, your history, and a look at how long symptoms have lasted, which is what separates persistent depressive disorder from a shorter major depressive episode.
Can high-functioning depression turn into major depression?
It can. When chronic low-grade depression goes unaddressed, the risk of a full major depressive episode rises, and the combination is sometimes called "double depression." Persistent symptoms also carry real cumulative costs to health, relationships, and safety. That is why duration matters: a low mood that has quietly persisted for years is a reason to get evaluated, not to wait for a crisis.
About the Author
Dr. Kiesa Kelly is a licensed clinical psychologist and the founder of ScienceWorks Behavioral Healthcare. Her background includes more than two decades of work in psychological assessment and evidence-based treatment, with particular depth in evaluating mood conditions like depression — where distinguishing a chronic, low-grade presentation from an acute major episode is often the key clinical question.
Dr. Kelly built ScienceWorks as a telehealth-forward practice serving Tennessee, with a clinical team specializing in assessment and evidence-based care for depression, anxiety, trauma, OCD, ADHD, and autism across adults and adolescents. Every article on this site is reviewed by a licensed clinician for accuracy before publication.
References
1. Persistent Depressive Disorder. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; updated 2024. https://www.ncbi.nlm.nih.gov/books/NBK541052/
2. Major Depressive Disorder. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK559078/
3. High-functioning depression: a hidden burden demanding clinical recognition. BJPsych Bulletin. 2025. https://www.cambridge.org/core/journals/bjpsych-bulletin/article/highfunctioning-depression-a-hidden-burden-demanding-clinical-recognition/5AE1AF5B7583F38C0DBDF1875D705E5C
4. Understanding High-Functioning Depression in Adults. Cureus. 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC11831407/
5. American Psychological Association. Clinical Practice Guideline for the Treatment of Depression Across Three Age Cohorts. 2019. https://www.apa.org/depression-guideline
6. National Institute for Health and Care Excellence (NICE). Depression in adults: treatment and management. NICE guideline [NG222]. 2022. https://www.nice.org.uk/guidance/ng222
7. Enduring effects of psychotherapy, antidepressants and their combination for depression: a systematic review and meta-analysis. Frontiers in Psychiatry. 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC11632389/
8. Kroenke K, Spitzer RL, Williams JBW. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606-613. https://pmc.ncbi.nlm.nih.gov/articles/PMC1495268/
9. Parker G, Malhi GS. Persistent Depression: Should Such a DSM-5 Diagnostic Category Persist? Canadian Journal of Psychiatry. 2019. https://journals.sagepub.com/doi/10.1177/0706743718814429
10. American Psychiatric Association. Persistent Depressive Disorder (DSM-5-TR fact sheet). https://www.psychiatry.org/getmedia/fd3dfaad-d409-4e94-8605-0350adec5b91/APA-DSM5TR-PersistentDepressive.pdf
11. CBASP in the Treatment of Persistent Depressive Disorder (editorial). Frontiers in Psychiatry. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8716920/
12. Centers for Disease Control and Prevention, National Center for Health Statistics. Depression Prevalence in Adolescents and Adults: United States. NCHS Data Brief. https://www.cdc.gov/nchs/products/databriefs/db527.htm
Disclaimer
This article is for informational and educational purposes only and is not a substitute for professional medical or mental health advice, diagnosis, or treatment. Reading it does not create a clinician-patient relationship. If you are struggling with your mood or safety, please reach out to a qualified professional. If you are in crisis or thinking about harming yourself, call or text 988 (the Suicide and Crisis Lifeline) in the United States, or go to your nearest emergency room.