
Perimenopause Burnout: When Mental Load and Hormonal Shifts Collide
- Kiesa Kelly

- 4 hours ago
- 13 min read
Last reviewed: 07/13/2026
Reviewed by: Dr. Kiesa Kelly
You are doing everything you have always done — running the household, holding down the job, remembering the birthdays and the permission slips — but somewhere in your late 30s or 40s it started costing far more than it used to. The words you want go missing mid-sentence. The mental to-do list that once felt manageable now feels like a weight you cannot set down. You are more tired than the day explains, more irritable than you want to be, and quietly afraid that something is wrong with you.
Perimenopause burnout is what happens when two things collide: the very real cognitive and emotional load women carry, and a brain that is temporarily working with less of the estrogen it relies on. It is not a character flaw, and it is not "just stress." Understanding why it happens — and when it is worth getting evaluated — can replace self-blame with something you can actually act on.
In this article, you'll learn:
What perimenopause burnout is, and why "brain fog" and "burnout" are really one story
The signs it shows up as in daily life, in the brain, and in your mood
The hormonal neurobiology behind it — estrogen, the hippocampus, and cognitive capacity
How PMDD and perimenopause overlap, and how to tell them apart
What actually helps, what to be cautious of, and which decisions belong to a medical provider
When cognitive or mood changes warrant a mental-health assessment
The core tension for most women is this: is this a sign that I am failing, or a sign that my brain and body are going through a real transition that deserves real support? The honest answer is the second one — and this article is built to help you act on it.
What perimenopause burnout actually is
Perimenopause is the stretch of years leading up to menopause, when the ovaries' production of estrogen begins to fluctuate — often starting in the late 30s or 40s, with the average age of menopause around 51 [1]. Clinically, it spans the "menopausal transition" and the first year after your final period [2]. Estrogen in this phase does not glide gently downward; it swings unpredictably, sometimes higher than usual and sometimes sharply lower, week to week.
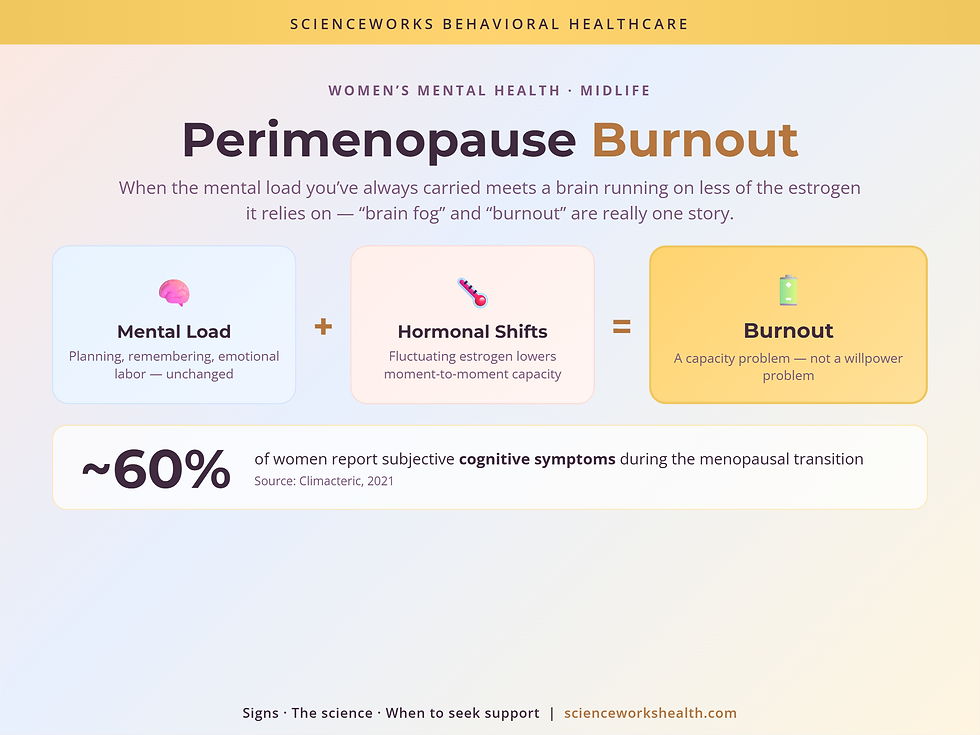
Perimenopause burnout is the experience of running your normal cognitive and emotional load on that unstable hormonal supply. The load itself — the planning, the anticipating, the emotional labor, the "who needs what and when" that so often falls to women — has not changed. What has changed is the brain's moment-to-moment capacity to carry it. When capacity drops while demand stays high, the result feels like burnout: depletion, overwhelm, and a sense that you are failing at things you used to do easily. If you are already stretched thin, evidence-based specialized therapy can help you sort out what is hormonal, what is situational, and what is treatable.
Let me clear up three misconceptions early, because they are often what keeps women stuck.
"If I am burning out, I am just not coping well enough." In reality, there is a measurable biological contributor here. Fluctuating estrogen affects brain regions that support memory, attention, and mood, and up to roughly 60% of women report subjective cognitive symptoms during the transition [3]. This is not weakness; it is neurobiology meeting a heavy load.
"Brain fog and burnout are two separate problems." They are really the same story told from two angles. Brain fog is the reduced-capacity side; burnout is what that reduced capacity feels like when it meets an unrelenting mental load. Competing articles tend to silo them — treating "menopause brain fog" and "midlife burnout" as unrelated. Holding them together is what makes the picture make sense.
"Cognitive changes now mean early dementia." For most women, they do not. The dips in memory and processing speed seen during perimenopause are typically transient and tend to recover after the final period [3][8]. Persistent or worsening changes still deserve evaluation — but the default story is transition, not decline.
How it shows up
Perimenopause burnout rarely announces itself as one dramatic symptom. It shows up as a pattern across your cognition, your mood, and your body.
Picture a Tuesday. You walk into the kitchen with a clear purpose and stand there, blank, unable to retrieve why. In a meeting, the exact word you need — one you have used a thousand times — simply will not come, and you cover with a vaguer one and hope no one noticed. By late afternoon you are running on fumes, snapping at the people you love most, then lying awake at 3 a.m. with your heart going while the day's undone tasks scroll past. None of these on its own is alarming. Together, week after week, they are the texture of perimenopause burnout.
Or picture the invisible-load version. You are the one who remembers that the dentist is Thursday, that your mother's prescription needs refilling, that the field trip needs cash, that the project at work is due before the long weekend. You have always carried this quietly and well. Now each item feels heavier, and the act of holding all of them at once — the very thing you were good at — is what leaves you depleted before the real work even starts. The tasks did not multiply. Your reserve to hold them shrank.
On the mood side, women often describe a shorter fuse, waves of anxiety that seem to come from nowhere, tearfulness that does not match the trigger, and a flatness or loss of enthusiasm that can shade into depression. A large cohort of perimenopausal and menopausal women seeking help reported very high rates of exactly these symptoms — memory problems, difficulty concentrating, irritability, and feeling tense or on edge — clustering together rather than appearing one at a time [5]. Because these mood symptoms overlap with clinical depression and anxiety, it is worth checking them directly; a brief depression screener and an anxiety screener can help you and a clinician see whether a treatable mood or anxiety condition is riding alongside the hormonal shift.
Key takeaway 🔋 Perimenopause burnout is a capacity problem, not a willpower problem: the mental load stayed the same while your brain's moment-to-moment reserve dropped.
How it's assessed
There is no single blood test that says "this is perimenopause burnout." Because hormone levels swing so much day to day, a one-time lab draw often cannot confirm the stage on its own — which is why clinicians lean on your symptom pattern and menstrual history alongside any testing [2]. A thoughtful evaluation separates three overlapping threads: the hormonal transition itself, a possible mood or anxiety condition, and the cognitive symptoms — then asks how much each is contributing.
From the behavioral-health side, this is where a structured psychological assessment earns its place. It can characterize the mood and cognitive picture, rule in or out depression and anxiety, and clarify whether what you are experiencing is proportionate to the transition or something that needs its own treatment. Because a clinical psychologist like Dr. Kiesa Kelly is not a physician, the assessment stays in its lane: it addresses the psychological and cognitive picture and coordinates with your medical provider for anything hormonal or medication-related.
Key takeaway 🧩 A good workup untangles three threads at once — the hormonal transition, a possible mood or anxiety disorder, and the cognitive symptoms — rather than forcing you to pick one.
Why it happens: the hormonal neurobiology
Estrogen is not only a reproductive hormone. In the brain, estradiol helps regulate synaptic plasticity, supports the hippocampus (a hub for memory), influences cerebral blood flow, and shapes how neurons use glucose for energy [6][7]. It also modulates the serotonin and dopamine systems that steady mood and motivation [7]. When estrogen is plentiful and stable, these systems hum along in the background. When it fluctuates and dips, the effects become noticeable.
Neuroimaging work led by researchers studying the menopause transition has shown measurable shifts across it — changes in gray matter volume and in how parts of the brain use glucose for fuel — alongside signs that the brain adapts to a lower-estrogen environment over time [6]. That word, adapts, matters: it is the neural basis for why the cognitive dip is usually temporary. The brain is recalibrating, not breaking.
This is also where "brain fog" and "burnout" fuse mechanistically. Reduced estrogen support means each cognitive task — holding a number in mind, finding a word, switching between demands — costs a little more effort. Multiply that small extra cost across a day full of demands, and the reserve you used to run on is gone by dinner. The fog is the per-task cost; the burnout is the cumulative bill.
It is worth being honest about the state of the evidence. One recent study following older adults found that women who recalled more perimenopausal symptoms — including brain fog, mood changes, and weight changes — showed somewhat greater later-life cognitive and behavioral change, and that estrogen-based menopause hormone therapy appeared to soften that link [4]. This is an emerging association from recalled symptoms, not proof that perimenopause causes long-term decline, and it should be read as a reason to take symptoms seriously, not as a cause for alarm.
Key takeaway 🌡️ Fluctuating estrogen raises the "cost" of everyday thinking; brain fog is that per-task cost, and burnout is the cumulative bill by day's end.
PMDD and perimenopause: overlapping, not identical
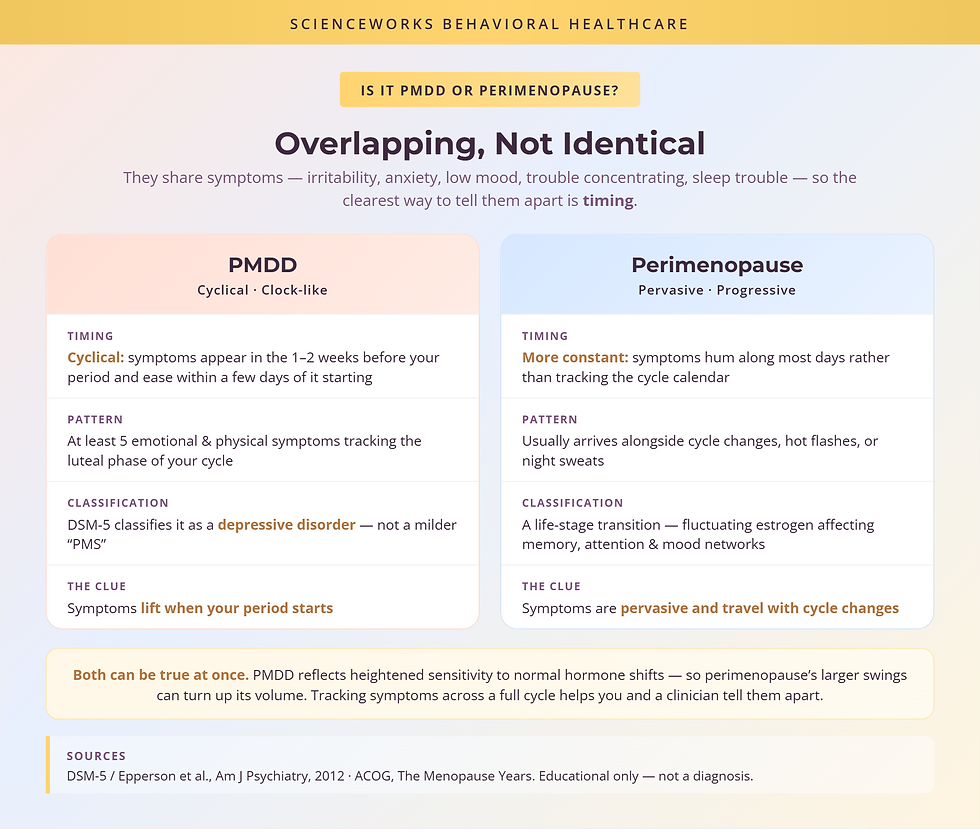
One of the most confusing overlaps in this stage is between perimenopause and premenstrual dysphoric disorder (PMDD). They share symptoms — irritability, anxiety, low mood, trouble concentrating, sleep disruption — so it is genuinely hard to tell them apart from the inside.
The distinguishing feature is timing. PMDD is a cyclical, luteal-phase condition: at least five emotional and physical symptoms appear in the one-to-two weeks before your period and then ease within a few days of it starting. Because of that pattern and its severity, the DSM-5 classifies PMDD as a depressive disorder rather than a milder "PMS" [9]. Perimenopause symptoms, by contrast, are more constant and are usually accompanied by menstrual-cycle changes, hot flashes, or night sweats [1].
Here is the part that trips people up: the two can coexist, and PMDD can worsen during perimenopause. PMDD reflects heightened sensitivity to normal hormone shifts, so the larger, more chaotic swings of perimenopause can turn up the volume — which is why many women report their premenstrual weeks feeling harder in their late 30s and 40s [9]. If you want a deeper look at how these hormonal patterns can also braid together with attention and executive-function changes, our companion piece on PMDD, perimenopause, and shifting patterns walks through how to spot the shifts.
The distinguishing pattern: PMDD costs are cyclical and clock-like — they track the calendar of your cycle and lift when your period starts. Perimenopause costs are pervasive and progressive — they hum along most days and travel with cycle changes and vasomotor symptoms.
Key takeaway 📆 Track the timing: cyclical, pre-period spikes that lift with menstruation point toward PMDD, while more constant symptoms with cycle changes point toward perimenopause — and both can be true at once.
What actually helps — and what belongs to a medical provider
There is no single fix, but there is real leverage. The behavioral-health side focuses on capacity and load:
Protect sleep first. Sleep loss amplifies every cognitive and mood symptom here, so stabilizing it often pays the largest dividend.
Lower the invisible load where you can. Offloading, sharing, and dropping non-essential mental tasks is not giving up; it is matching demand to current capacity.
Treat co-occurring depression and anxiety directly. When a mood or anxiety condition is riding alongside the transition, treating it — with therapy, and sometimes medication prescribed by a medical provider — lifts a large share of the burden. For PMDD specifically, SSRIs are a well-established first-line treatment and can sometimes be taken only in the luteal phase rather than daily [10].
Build recovery in, not just around. Short, real breaks that let the brain reset beat pushing through on an empty tank.
Now the boundary that matters most. Decisions about hormone therapy, HRT, or any prescription belong with a medical provider — your OB-GYN or primary care physician — not a psychologist. Systemic estrogen therapy is the most effective treatment for perimenopause-related vasomotor symptoms, and some women find it also eases cognitive and mood symptoms, but it carries individual risks and benefits that require medical evaluation [11]. Be cautious of anyone — a supplement marketer, a wellness influencer, or any provider — promising to "cure" perimenopause or guaranteeing a specific outcome. The honest picture is that good care is individualized and coordinated, not one-size-fits-all.
When to get evaluated
Use this simple decision heuristic. If your hardest days are cyclical — clustering before your period and lifting once it starts — bring a PMDD lens and a symptom diary to your provider. If your symptoms are pervasive — most days, alongside cycle changes or hot flashes — the perimenopause lens fits better. If both feel true, do not talk yourself out of that; the two commonly coexist, and naming both is the most honest starting point.
Layer a second rule on top for the mental-health piece: if low mood, anxiety, or cognitive symptoms last most days for two weeks or more, interfere with work or relationships, or come with hopelessness — and always if you have thoughts of self-harm — that is the threshold to seek an assessment rather than wait it out. Our mental-health screening tools are a low-stakes first step, and you can reach out to us to talk through what a full evaluation would involve.
If you do book an evaluation, these questions help you get what you need:
Scope: Will this assessment look at mood, anxiety, and the cognitive symptoms, or only one of them?
Methodology: How do you tell apart what is hormonal, what is a mood or anxiety disorder, and what is normal transition?
History: What information about my cycle, symptom timing, and history will you gather to make that distinction?
Output: What will I actually walk away with — a diagnosis, specific recommendations, a plan I can use?
Coordination: If hormone therapy or medication might help, how will you coordinate with my OB-GYN or primary care doctor?
Key takeaway 📋 Bring a cycle-tracked symptom diary and these five questions to your appointment — they turn a vague "I feel off" into something a clinician can actually work with.

Next step — getting support
Perimenopause burnout is real, it has a biology, and it is not a verdict on your worth or your competence. What you are carrying is heavy, and your brain is doing it with less of the fuel it is used to — for now. Naming that clearly is the first step; getting the right kind of support is the second.
Navigating a women's-health or hormonal change?
Hannah Pollok works at the intersection of physical and mental health — hormones, reproductive changes, and the mood and cognitive shifts that come with them.
Frequently Asked Questions
How do I know if it's PMDD or perimenopause?
The clearest clue is timing. PMDD symptoms follow a cyclical pattern — they appear in the one to two weeks before your period and ease within a few days of it starting. Perimenopause symptoms tend to be more constant and often arrive alongside cycle changes, hot flashes, or night sweats. The two can also overlap, and PMDD can intensify during perimenopause, so tracking your symptoms across a full cycle helps you and a clinician tell them apart.
Why does my usual mental load feel so much heavier now?
Because the fuel your brain runs on has become less steady. The same planning, remembering, and emotional labor now costs more effort per task, as fluctuating estrogen affects the memory and attention networks you rely on, so your usual reserve runs out sooner. The load did not grow — your moment-to-moment capacity to carry it dipped. That gap is what perimenopause burnout feels like, and it is a capacity problem, not a failure of effort or will.
What helps perimenopause burnout and brain fog?
Start by naming what is fixed and what is flexible. Protecting sleep, building in real recovery time, lowering the invisible mental load you carry, and treating any co-occurring depression or anxiety all help the brain work with the capacity it has. For some women, medical options such as hormone therapy also ease cognitive and mood symptoms — but those are decisions to make with a medical provider like your OB-GYN or primary care doctor, not a psychologist.
Are perimenopause cognitive changes permanent?
For most women, no. Research on the menopause transition suggests that dips in memory and processing speed are often temporary and tend to recover in the years after the final period. Even so, persistent or worsening changes deserve a proper evaluation rather than reassurance alone, so that treatable contributors — sleep, mood, thyroid, or medication effects — are not quietly missed.
When should I get a mental-health assessment in perimenopause?
Consider an assessment when low mood, anxiety, or cognitive symptoms last most days for two weeks or more, disrupt work or relationships, or come with hopelessness or thoughts of self-harm. Brief screeners for depression and anxiety are a useful first step, and a psychologist can help sort out how much is hormonal, how much reflects a mood or anxiety condition, and what would actually help.
About the Author
Dr. Kiesa Kelly is a licensed clinical psychologist with more than 20 years of experience in psychological assessment and evidence-based treatment, and the founder of ScienceWorks Behavioral Healthcare. Her work centers on careful differential assessment — distinguishing mood and anxiety conditions, cognitive changes, and life-stage transitions so that people get an accurate picture and a usable plan, which is exactly the kind of untangling perimenopause burnout requires.
Dr. Kelly is a PhD clinical psychologist, not a physician. In practice, that means her role is to assess and treat the psychological and cognitive side of the perimenopause picture and to coordinate with medical providers for anything involving hormones or medication. ScienceWorks is a telehealth-forward practice serving Tennessee, with an in-person option in Nashville, and every article is reviewed by a licensed clinician for accuracy before publication.
References
1. American College of Obstetricians and Gynecologists. The Menopause Years. https://www.acog.org/womens-health/faqs/the-menopause-years
2. Harlow SD, Gass M, Hall JE, et al. Executive summary of the Stages of Reproductive Aging Workshop + 10: addressing the unfinished agenda of staging reproductive aging. J Clin Endocrinol Metab. 2012. https://pmc.ncbi.nlm.nih.gov/articles/PMC3340903/
3. Scientific insights into brain fog during the menopausal transition. Climacteric. 2021. https://www.tandfonline.com/doi/full/10.1080/13697137.2021.1942700
4. Cognitive and behavioral decline predicted by perimenopausal symptoms: a CAN-PROTECT study. Alzheimer's & Dementia. 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC11710710/
5. Prevalence of cognitive and mood-related symptoms in a large cohort of perimenopausal and menopausal women. BJPsych Open. 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC11738833/
6. Mosconi L, Berti V, Dyke J, et al. Menopause impacts human brain structure, connectivity, energy metabolism, and amyloid-beta deposition. Scientific Reports. 2021. https://www.nature.com/articles/s41598-021-90084-y
7. Estrogen, menopause, and Alzheimer's disease: understanding the link to cognitive decline in women. Frontiers in Molecular Biosciences. 2025. https://www.frontiersin.org/journals/molecular-biosciences/articles/10.3389/fmolb.2025.1634302/full
8. Cognition and the menopause transition: cross-sectional evidence from a large community cohort. npj Women's Health. 2026. https://www.nature.com/articles/s44294-026-00132-z
9. Epperson CN, Steiner M, Hartlage SA, et al. Premenstrual dysphoric disorder: evidence for a new category for DSM-5. American Journal of Psychiatry. 2012. https://psychiatryonline.org/doi/10.1176/appi.ajp.2012.11081302
10. Harvard Health Publishing. Treating premenstrual dysphoric disorder. https://www.health.harvard.edu/womens-health/treating-premenstrual-dysphoric-disorder
11. American College of Obstetricians and Gynecologists. Management of Menopausal Symptoms (Practice Bulletin). https://www.acog.org/clinical/clinical-guidance/practice-bulletin/articles/2014/01/management-of-menopausal-symptoms
Disclaimer
This article is for informational and educational purposes only and is not a substitute for professional medical or mental-health advice, diagnosis, or treatment. It does not establish a provider-patient relationship. Decisions about hormone therapy, medication, and other medical treatments should be made with a qualified medical provider such as your OB-GYN or primary care physician. If you are experiencing thoughts of self-harm or are in crisis, call or text 988 (the Suicide and Crisis Lifeline) or go to your nearest emergency room. Always seek the advice of a qualified health provider with any questions you may have about a medical or psychological condition.