
Complex PTSD vs. PTSD: Key Differences in Symptoms & Care
- Kiesa Kelly

- Jun 2
- 16 min read
Updated: Jul 17
Last reviewed: 06/02/2026
Reviewed by: Dr. Kiesa Kelly

If you have read about post-traumatic stress disorder and felt like the description only captured part of your experience, you are not alone. Many people recognize the nightmares, the flashbacks, and the constant feeling of being on guard — but they also carry something the standard PTSD picture rarely names: a deep, lasting sense of being broken, a hair-trigger emotional system, and relationships that feel impossible to trust. That fuller picture has a name. It is called Complex PTSD, and understanding how it differs from classic PTSD can change how you make sense of your own history and what kind of help actually fits.
This is an educational guide, not a diagnostic tool. Trauma diagnoses are made by a qualified clinician through careful assessment, never by reading an article. But knowing the difference between PTSD and complex PTSD helps you ask better questions, and it explains why two people with trauma histories can need very different paths to heal.
In this article, you'll learn:
The core difference between PTSD and complex PTSD in plain language
What classic, single-incident PTSD looks like
The three additional symptom clusters that define complex PTSD
Why prolonged, repeated trauma — not a one-time event — tends to drive C-PTSD
How the ICD-11 and DSM-5 handle the diagnosis differently, and how clinicians actually assess it
Why the distinction reshapes treatment into a slower, phase-based arc
Short answer — the core difference between PTSD and complex PTSD
PTSD and complex PTSD share the same foundation. Both involve re-experiencing a traumatic event, avoiding reminders of it, and living with a heightened sense of current threat. The difference is what complex PTSD adds on top of that foundation.
Complex PTSD includes all the core symptoms of PTSD, plus three additional patterns that show up in how you relate to your own emotions, your sense of self, and other people. The World Health Organization, in its ICD-11 diagnostic system, calls these added patterns disturbances in self-organization [1]. In everyday terms, they are trouble regulating emotion, a persistent negative self-view often rooted in shame, and ongoing difficulty feeling safe and connected in relationships.
There is also a difference in cause. PTSD can follow a single traumatic event — a car crash, an assault, a disaster. Complex PTSD typically develops after trauma that is prolonged, repeated, and hard or impossible to escape, such as childhood abuse, long-term domestic violence, or captivity [2]. That distinction is not just academic. It shapes the symptoms, and it shapes treatment. If you are looking for trauma-focused care that takes this fuller picture seriously, our complex PTSD therapy in Tennessee is built around exactly this kind of layered trauma history.
It also helps to be precise about what "trauma" even means here, because the word gets stretched to cover everything from a stressful week to a life-threatening event. If you want the broader framing first, our overview of what trauma means in mental health walks through how trauma differs from ordinary stress — useful context for everything that follows.
📌 Key takeaway: Complex PTSD is not a more severe version of the same thing. It is PTSD plus lasting changes in emotion regulation, self-worth, and relationships — usually following repeated trauma rather than a single event.

What PTSD is: single-incident trauma and the classic symptom triad
Post-traumatic stress disorder is what can develop after you are exposed to actual or threatened death, serious injury, or sexual violence — either directly, by witnessing it, or by learning it happened to someone close to you. The classic picture, recognized across both the ICD-11 and the American DSM-5-TR, organizes around three core features [3].
The first is re-experiencing. The trauma intrudes on the present through nightmares, vivid flashbacks, or unwanted memories that arrive with the emotional and physical intensity of the original event. The U.S. Department of Veterans Affairs National Center for PTSD describes these intrusions as a hallmark of the disorder [4].
The second is avoidance. You steer away from people, places, conversations, or even thoughts that bring the trauma back. Someone who survived a serious car accident may stop driving on highways. A combat veteran may avoid crowds or fireworks.
The third is a sense of current threat — what clinicians call hyperarousal. Your nervous system stays braced for danger. You startle easily, struggle to sleep, feel irritable, and scan every room for exits. The brain's threat-detection system is essentially stuck in the "on" position [5]. If you are curious about what is happening at the level of brain circuitry, our deeper dive into the neuroscience of PTSD unpacks how trauma reshapes the alarm system.
Consider a concrete example. A man is mugged at knifepoint walking home one night. In the months after, he cannot shake the memory — it floods back whenever he passes that block, and sometimes for no clear reason at all. He starts taking a long detour to avoid the street, stops going out after dark, and lies awake replaying what happened. His partner notices he flinches when someone walks up behind him. This is a recognizable PTSD presentation: a single, identifiable event, followed by re-experiencing, avoidance, and a body that will not stand down.
Crucially, in this kind of PTSD, the person's underlying sense of who they are often stays intact. He knows the mugging was not his fault. He still trusts the people close to him. His symptoms are anchored to a specific threat. That preserved core is part of what distinguishes classic PTSD from its complex counterpart.
What complex PTSD adds
Complex PTSD starts from that same PTSD foundation — re-experiencing, avoidance, and a sense of threat are all present — but it does not stop there. The ICD-11 defines C-PTSD as PTSD plus three additional symptom clusters, grouped together as disturbances in self-organization [1]. These are the patterns that the single-incident PTSD picture leaves out, and they are often the ones that cause people the most quiet, ongoing distress.
Emotion regulation, self-worth, and relational difficulty
The first added cluster is affect dysregulation — trouble managing emotions. This can look like emotional reactions that feel far bigger than the situation warrants, a long time to calm down once upset, or the opposite: feeling numb, shut down, or cut off from emotion entirely. Small frustrations can tip into overwhelm. Many people describe it as living without a working volume knob.
The second cluster is a persistently negative self-concept. This is more than low self-esteem. It is a bone-deep belief that you are worthless, damaged, or fundamentally different from other people — a belief that feels like fact rather than feeling. People with complex PTSD often carry pervasive guilt and shame about the trauma itself, even when they were not responsible for it [6].
The third cluster is disturbance in relationships. You may find it consistently hard to feel close to others, to trust, or to sustain connection. Some people avoid relationships altogether; others get pulled into intense, unstable ones. The underlying difficulty is the same: relationships feel unsafe, because for a long time they were.
Here is what these three clusters can look like woven into a daily life. A woman who grew up with an unpredictable, frightening parent now functions well at work — she is competent, even high-achieving. But underneath, she is exhausted. A mildly critical email from her boss can send her into a spiral of self-loathing that lasts for days. She is certain, in a way she cannot argue herself out of, that she is a fraud who will eventually be found out. When her partner gets close, she feels a pull to push them away before they can leave first. None of this maps onto a single, nameable event. It is the residue of years.
Or consider a man who was bullied and emotionally neglected throughout childhood. He has no flashbacks in the cinematic sense — no vivid replay of one bad day. Instead, certain situations flood him with the feeling of being small, helpless, and humiliated, with no clear memory attached. A colleague raising their voice in a meeting can drop him straight back into that old emotional state. These are emotional flashbacks, and they are one of the most recognizable experiences in complex PTSD [7].
The distinguishing pattern: PTSD's costs are anchored to a remembered threat, while complex PTSD's added costs are identity-based and relational — they show up as who you believe you are and how unsafe closeness feels, not just as fear of a specific event.
Why C-PTSD is rooted in shame, not just fear
Classic PTSD is, at its core, a disorder of fear. The threat system learned that the world is dangerous, and it keeps firing. Treatment that helps the fear system update — learning at a gut level that the danger has passed — is often enough to make a meaningful difference.
Complex PTSD runs on a second engine: shame. When trauma is prolonged and happens within relationships you depend on — especially in childhood — the lesson the developing mind absorbs is not only "the world is dangerous." It is "the danger is about me. There is something wrong with me, and that is why this is happening." That belief gets wired in early and feels like bedrock truth.
This matters because fear and shame respond to different things. You can help a fear response settle by safely revisiting the memory until the body learns it is over. Shame does not work that way. A person can fully process a traumatic memory and still believe they are worthless, because the shame was never about the event — it was about the self that the event taught them to be. Mechanism-wise, this is the key reason complex PTSD needs more than memory processing. Fear-focused exposure addresses the re-experiencing engine; the self-concept and relational engines require their own, often slower, repair work [8].
🧩 Key takeaway: If you have processed your trauma but still feel fundamentally defective, you are not failing at recovery. Shame-based self-concept is a separate target from fear-based memory, and it asks for its own kind of work.
A common misconception is worth naming directly here. Complex PTSD is just more severe PTSD. In reality, severity and complexity are different axes. A single-event PTSD case can be extremely severe and disabling. A complex PTSD case is defined not by how intense the fear is, but by the additional domains affected — emotion, identity, and relationships. Two people can have the same level of distress and still need different treatment maps.
Another misconception: if I cannot remember much of my childhood, I cannot have complex PTSD. Actually, gaps in autobiographical memory are common after prolonged early trauma, and the absence of crisp narrative memories does not mean the trauma did not register. The nervous system and self-concept can carry what the timeline cannot.
And a third: complex PTSD means I am beyond help. The word "complex" describes the structure of the symptoms, not the prognosis. Complex PTSD is treatable, and people recover meaningful stability, self-worth, and connection with the right, appropriately paced care [9].
Why it's prolonged, repeated trauma that drives C-PTSD
The defining feature in the cause of complex PTSD is not the type of trauma so much as its shape over time. The ICD-11 specifies that C-PTSD typically follows events that are prolonged or repetitive and from which escape is difficult or impossible [2]. Think of chronic childhood abuse, long-term domestic violence, repeated exploitation, or captivity — situations where the threat is not a single shock but an ongoing condition of life.
Repetition does something a single event usually does not. When trauma happens over and over within important relationships, the mind adapts to survive inside the danger rather than recover after it. A child cannot leave a frightening home, so they adapt — by going numb, by blaming themselves (which at least preserves the hope that a "good enough" child could make it stop), by reading the emotional weather constantly. Those adaptations are intelligent responses to an impossible situation. The problem is that they outlast the situation, hardening into the emotion-regulation, self-worth, and relationship patterns that define complex PTSD [10].
Timing adds weight. When prolonged trauma occurs during childhood and adolescence, it lands on a brain and a sense of self that are still under construction. The Adverse Childhood Experiences research has shown, across very large samples, that repeated early adversity is associated with significantly elevated risk for a range of mental and physical health difficulties later in life [11]. That does not mean a hard childhood guarantees complex PTSD — most people are remarkably resilient — but it explains why developmental, relational trauma is the most common soil for it.
This is also why two trauma histories can look so different. Single-incident trauma leaves a wound on an intact structure. Prolonged developmental trauma shapes the structure as it forms. Both deserve care; they simply are not the same injury.
🌡️ Key takeaway: It is the prolonged and inescapable nature of the trauma — often, though not only, in childhood — that adds the self-organization symptoms. The repetition is what turns survival adaptations into lasting patterns.
Diagnosis: ICD-11 vs. DSM-5, and how clinicians actually assess it
This is the question that brings many people to search in the first place: is complex PTSD a real diagnosis? The honest answer is that it depends on which diagnostic system you are looking at — and getting this right matters.
The ICD-11, the World Health Organization's international classification used across much of the world, formally recognizes Complex PTSD as a distinct diagnosis, separate from PTSD, with its own defined criteria built around the core PTSD symptoms plus the three disturbances in self-organization [1]. Internationally, C-PTSD is an official, codeable diagnosis.
The DSM-5-TR, published by the American Psychiatric Association and used most commonly in the United States, does not list Complex PTSD as a separate diagnosis [12]. Instead, the DSM keeps a single, broader PTSD category. Some features that the ICD-11 assigns to C-PTSD are addressed within the DSM through a dissociative subtype of PTSD and through PTSD's negative-mood and self-concept criteria, but there is no standalone "Complex PTSD" code in the DSM system [12]. The U.S. Department of Veterans Affairs National Center for PTSD explains this split plainly: the term is widely used and clinically meaningful, even though the DSM does not classify it separately [13].
So both can be true at once. A reader can be told by one clinician that they have "complex PTSD" and by another that they have "PTSD with prominent emotion-regulation and self-concept symptoms," and neither is wrong — they are speaking different diagnostic languages about the same lived reality.
How do clinicians actually assess this in practice? Not from a single questionnaire. A careful trauma evaluation combines a structured clinical interview, a detailed trauma and developmental history, and validated measures. Self-report screeners — including the PCL-5 for PTSD symptoms and, where complex symptoms are suspected, the International Trauma Questionnaire designed specifically around the ICD-11 C-PTSD criteria — can structure the conversation and track change over time [14]. But a screener is a starting point, never a diagnosis. You can see how we think about that first step on our mental health screening page. The diagnosis itself comes from a clinician integrating the whole picture.
If you are preparing to talk to a provider, here are concrete questions worth asking:
Do you assess for the emotion-regulation, self-worth, and relational symptoms of complex PTSD — not just the core PTSD symptoms?
How do you gather developmental history if I do not have clear childhood records or memories?
Do you use a measure built around the ICD-11 complex PTSD criteria, such as the International Trauma Questionnaire?
What will I actually receive after the evaluation — a label, a formulation of what is driving my symptoms, and specific treatment recommendations?
📋 Key takeaway: ICD-11 recognizes Complex PTSD as its own diagnosis; DSM-5-TR does not, folding related features into PTSD and its dissociative subtype. A real assessment is an interview plus history plus validated measures — never a single test.
Why the distinction changes treatment: a phase-based, longer arc
Here is where the difference stops being a labeling debate and starts mattering for healing. The treatment that works well for single-incident PTSD is not, on its own, the right shape for complex PTSD.
For classic PTSD, trauma-focused therapies that process the memory directly — such as EMDR, prolonged exposure, or cognitive processing therapy — are first-line and often work efficiently [3]. You can read more about how trauma-focused therapy approaches this kind of memory work, and if you are weighing two of the most common options, our comparison of EMDR vs. CPT lays out how those two evidence-based approaches differ. When the self-concept and relational systems are intact, helping the fear response update can be enough.
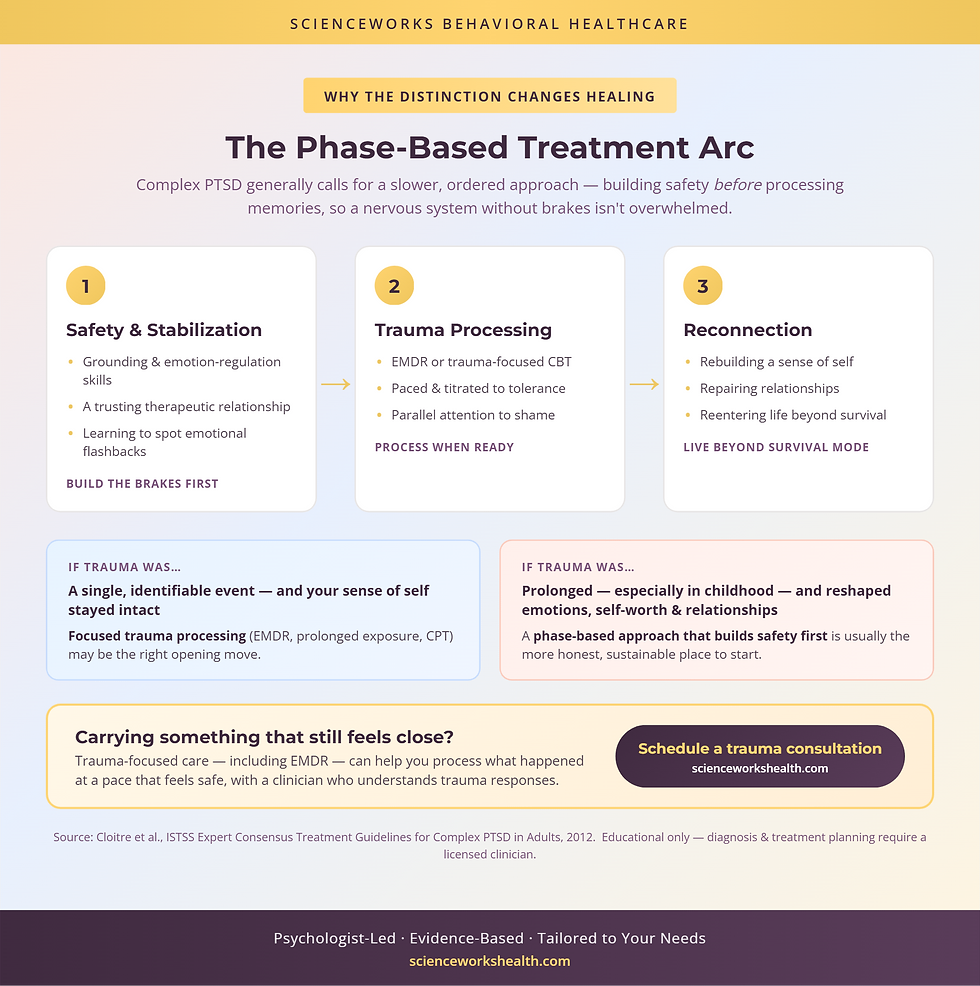
Complex PTSD generally calls for a phase-based approach over a longer timeline, an arc that has become the consensus framework in expert guidance on complex trauma [8]. The logic is straightforward: someone with significant affect dysregulation cannot safely dive straight into processing their worst memories, because doing so can flood a nervous system that does not yet have the brakes to handle it.
The first phase focuses on safety and stabilization — building grounding skills, emotion-regulation tools, and a trusting therapeutic relationship. For someone whose core wound is that relationships are dangerous, that relationship is part of the treatment, not just the container for it. Only once there is enough stability does the second phase move into trauma processing, using approaches like EMDR or trauma-focused CBT, but paced carefully and titrated to what the person can tolerate. A third phase focuses on reconnection — rebuilding a sense of self, repairing relationships, and reentering life beyond survival mode [8].
Compare two arcs to make this concrete. Someone with single-event PTSD after an assault might do a focused course of EMDR, process the memory over a defined number of sessions, watch the re-experiencing and avoidance recede, and finish with their self-worth and relationships essentially intact. Someone with complex PTSD from childhood abuse usually cannot start there. They may spend the early months learning to notice an emotional flashback and ground themselves out of it, gradually building enough internal safety to approach the memories at all — with steady, parallel attention to the shame-based self-concept that memory processing alone will not touch. The destination overlaps; the road is longer and differently ordered.
This is not a reason for discouragement. It is a reason to find care that recognizes which map you are on. Treatment that respects the phase-based arc tends to feel less overwhelming and more sustainable precisely because it does not ask you to process trauma before you are equipped to survive doing so.
🔋 Key takeaway: The decision heuristic is simple. If trauma was a single, identifiable event and your sense of self stayed intact, focused trauma processing may be the right opening move. If trauma was prolonged — especially in childhood — and it reshaped your emotions, self-worth, and relationships, a phase-based approach that builds safety first is usually the more honest and effective place to start.
Carrying something that still feels close?
Trauma-focused care — including approaches like EMDR — can help you process what happened at a pace that feels safe, with a clinician who understands trauma responses.
Frequently Asked Questions
Is complex PTSD an official diagnosis?
It depends on the diagnostic system. The World Health Organization's ICD-11 lists Complex PTSD as a distinct, formal diagnosis with its own criteria. The American DSM-5-TR does not — it keeps a single PTSD diagnosis and folds some related features into a dissociative subtype. So C-PTSD is formally recognized internationally, and many U.S. clinicians use it descriptively even though it is not a separate DSM code.
What's the main difference between PTSD and complex PTSD?
Both share the core PTSD symptoms — reliving the trauma, avoidance, and a constant sense of threat. Complex PTSD adds three more patterns ICD-11 calls disturbances in self-organization: trouble managing emotions, a deeply negative view of yourself often shaped by shame, and ongoing difficulty feeling safe or close in relationships. C-PTSD usually follows repeated or prolonged trauma rather than a single event.
What is an emotional flashback in complex PTSD?
An emotional flashback is a sudden return of the feelings from past trauma — fear, shame, helplessness, or panic — without a clear visual memory attached. Unlike a classic PTSD flashback, you may not picture the event at all; you just feel the way you felt then, often triggered by something small. Recognizing these as flashbacks, not present-day reality, is an early goal in trauma therapy.
Does complex PTSD always come from childhood trauma?
Not always, but it is strongly linked to prolonged trauma during development. Childhood abuse, neglect, or chronic instability are common roots because they shape self-worth and relationships while the brain is still forming. C-PTSD can also follow adult experiences that are repeated and hard to escape, such as domestic violence, trafficking, or captivity. The common thread is sustained, inescapable trauma — not its timing alone.
How is complex PTSD treated differently from PTSD?
Treatment for C-PTSD usually follows a phase-based arc over a longer timeline. Early work focuses on safety, grounding, and emotion-regulation skills before processing the trauma itself, because diving straight into memories can overwhelm someone with affect dysregulation. Trauma-focused approaches like EMDR or trauma-focused CBT are still used, but they are paced carefully and paired with steady attention to self-worth and relationships.
About the Author
Dr. Kiesa Kelly is a licensed clinical psychologist and the founder of ScienceWorks Behavioral Healthcare. Her background includes more than 20 years of experience in psychological assessment and evidence-based treatment, with particular depth in trauma, anxiety, and neurodevelopmental conditions across adults and adolescents. Her clinical training spans work at major universities and clinical settings, and her practice centers on careful, individualized assessment — the kind that distinguishes a single-incident trauma history from a complex, developmental one.
Dr. Kelly built ScienceWorks as a telehealth-forward practice serving Tennessee, with a clinical team specializing in trauma-focused care, including EMDR and phase-based treatment for complex trauma. Every article on this site is reviewed by a licensed clinician for accuracy before publication, reflecting the same standard of care the practice brings to the consulting room.
References
1. World Health Organization. International Classification of Diseases, 11th Revision (ICD-11): 6B41 Complex post traumatic stress disorder. 2024. https://icd.who.int/browse/2024-01/mms/en#585833559
2. Maercker A, Cloitre M, Bachem R, et al. Complex post-traumatic stress disorder. The Lancet. 2022;400(10345):60-72. https://doi.org/10.1016/S0140-6736(22)00821-2
3. Bisson JI, Wright LA, Jones KA, et al. Preventing the onset of post traumatic stress disorder. Clinical Psychology Review. 2021;86:102004. https://doi.org/10.1016/j.cpr.2021.102004
4. U.S. Department of Veterans Affairs, National Center for PTSD. PTSD basics: symptoms of PTSD. 2024. https://www.ptsd.va.gov/understand/what/ptsd_basics.asp
5. National Institute of Mental Health. Post-traumatic stress disorder. 2024. https://www.nimh.nih.gov/health/topics/post-traumatic-stress-disorder-ptsd
6. Karatzias T, Hyland P, Bradley A, et al. Risk factors and comorbidity of ICD-11 PTSD and complex PTSD: findings from a trauma-exposed population based sample of adults. Depression and Anxiety. 2019;36(9):887-894. https://doi.org/10.1002/da.22934
7. Cloitre M, Shevlin M, Brewin CR, et al. The International Trauma Questionnaire: development of a self-report measure of ICD-11 PTSD and complex PTSD. Acta Psychiatrica Scandinavica. 2018;138(6):536-546. https://doi.org/10.1111/acps.12956
8. Cloitre M, Courtois CA, Ford JD, et al. The ISTSS Expert Consensus Treatment Guidelines for Complex PTSD in Adults. International Society for Traumatic Stress Studies. 2012. https://istss.org/wp-content/uploads/2024/10/ISTSS_CPTSD-Position-Paper-Adults_FNL.pdf
9. Karatzias T, Murphy P, Cloitre M, et al. Psychological interventions for ICD-11 complex PTSD symptoms: systematic review and meta-analysis. Psychological Medicine. 2019;49(11):1761-1775. https://doi.org/10.1017/S0033291719000436
10. Herman JL. Complex PTSD: a syndrome in survivors of prolonged and repeated trauma. Journal of Traumatic Stress. 1992;5(3):377-391. https://doi.org/10.1002/jts.2490050305
11. Hughes K, Bellis MA, Hardcastle KA, et al. The effect of multiple adverse childhood experiences on health: a systematic review and meta-analysis. The Lancet Public Health. 2017;2(8):e356-e366. https://doi.org/10.1016/S2468-2667(17)30118-4
12. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR): Trauma- and Stressor-Related Disorders. 2022. https://doi.org/10.1176/appi.books.9780890425787
13. U.S. Department of Veterans Affairs, National Center for PTSD. Complex PTSD. 2024. https://www.ptsd.va.gov/professional/treat/essentials/complex_ptsd.asp
14. Brewin CR, Cloitre M, Hyland P, et al. A review of current evidence regarding the ICD-11 proposals for diagnosing PTSD and complex PTSD. Clinical Psychology Review. 2017;58:1-15. https://doi.org/10.1016/j.cpr.2017.09.001
Disclaimer
This article is for informational and educational purposes only and is not a substitute for professional medical or psychological advice, diagnosis, or treatment. Reading it does not establish a clinician-patient relationship. Complex PTSD and PTSD can only be diagnosed by a qualified professional through a comprehensive evaluation. If you are struggling with trauma, please reach out to a licensed clinician. If you are in crisis or thinking about harming yourself, call or text 988 to reach the Suicide and Crisis Lifeline in the United States, or contact your local emergency services.